Reductionism and Complex Systems Science Implications for Translation












")
































- Slides: 47
Reductionism and Complex Systems Science: Implications for Translation Research in the Health and Behavioral Sciences David G. Schlundt, Ph. D. Associate Professor of Psychology CRC Research Skills January 20, 2011
Overview NIH party line on translation research Problems with the party line Reductionism in modern science Problems with reductionism Complex systems science as an alternative Problems with complex systems science Examining the obesity epidemic as a real-life exemplar Integrating scientific approaches Implications for basic and applied research on obesity
What is Translation Research? Problem: basic research findings take years or decades to find their way into evidence-based practice Problem: Landmark clinical trials take years or decades to find their way into evidence-based practice Problem: The investment in basic research has not resulted in a corresponding improvement in health care delivery Goal: Translate the discoveries of basic scientific research into population level gains in health
NIH Road Map New Pathways to Discovery - unravel the complexity of biologic systems and their regulation Research Teams of the Future – break down the barriers to interdisciplinary and transdisciplinary research Re-engineering the Clinical Research Enterprise – bring more scientists into clinical research Solution: Clinical Science Translation Awards (CTSA) – infrastructure to support clinical and translation research at academic institutions
The T’s of translation T 1 – from bench to bedside Taking basic biological sciences and using them to create useful diagnostic tests, drugs, and therapies T 2 – from bedside to community Moving clinical research findings into evidence-based practice and looking at the impact on the public’s health These definitions: Were created by the basic scientists who run the NIH research enterprise Imagine a one-way flow of knowledge from basic research to improved health care Over simplify what is a complicated problem (how to improve human health)
Problems with the T 1 -T 2 vision The amount of resources at the NIH continues to be disproportionately allocated for basic research The basic scientists in charge have underestimated the difficulty and amount of time required to plan and execute translation research studies The clinical relevance of basic research findings is overestimated Translation research proposals are too often reviewed by basic scientists who review translation studies using their basic research framework Much greater improvement in population health could be achieved by improving current health care delivery – based standards of care that are not implemented Much greater improvement in population health could be achieved through health care reform
Meta Scientific Models There assumptions and frameworks behind the practice of science that drive the questions, the methodologies, and the development of new knowledge Philosophical Reductionism Offshoot of materialist philosophy Idea that one science (biology) can be reduced to the principals of another science (chemistry) Drive to find the most basic explanation There is potentially a single, underlying physical science that explains everything Methodological Reductionism The best scientific explanations come from breaking problems into their most fundamental elements Goal of science is to identify, isolate, and study basic causal mechanisms Approach is to create experiments in which only one parameter is allowed to vary so that its causal effect can be isolated Goal is to develop mechanistic explanations
Reductionism in Action Much “basic” research follows a reductionist framework in biological and behavioral sciences Reductionism Leads to increasing specialization Leads to problems being broken down into ever smaller problems Leads to a rapidly expanding base of knowledge in which the pieces are largely disconnected from each other Leads to new technologies and methodologies for achieving tighter and tighter control of ever smaller processes Even when the rationale for the research is an important clinical problem (e. g. , diabetes, depression, schizophrenia), the research itself ends up isolating only a small piece of the problem and studying it out of context
Reductionism Impedes Clinical Discoveries Reductionism is not the most efficient way to improve the physical and mental health of populations of human beings Most “breakthroughs” in basic health and neuroscience do not lead to new diagnostic or treatment approaches The overspecialization of disciplines makes it difficult for any one scientist to pull together enough basic knowledge to create meaningful new diagnostics or interventions Funding of basic science does not encourage interdisciplinary or transdisciplinary cooperation needed to create clinical applications
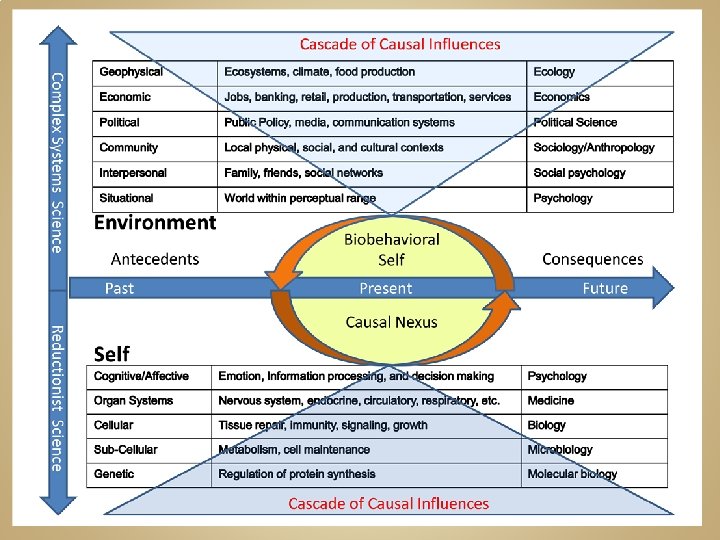
Unintended consequences of reductionism In reductionism, causality moves one way from low order phenomenon to higher order phenomenon Ignores the possibility of complex higher order systems exerting a causal influence on more basic lower order systems Biogenetic determinism moves explanation of social and behavioral problems to the genes Individual rather than social conditions or economic inequities is responsible for problems However, the individual is not responsible, the genes are responsible Many modern individuals have a sense of helplessness due to a naive reductionism (obesity and depression good examples) Much effort is put towards finding new drugs that will solve social/interpersonal/emotional/economic/political problems
Alternatives to Reductionism Holism – systems cannot be understood by taking them apart Emergent Properties – as components associate into systems, new properties of the systems emerge which cannot be predicted from the properties of the components (e. g. , hydrogen + oxygen water) Complex systems science – systems form hierarchies of increasing complexity and exhibit adaptive behavior at each level of analysis Homeostasis Feedback loops Cross-level linkages
http: //necsi. org/projects/mclemens/cs_char. gif
Problems with Complex systems Goals of science are the same (understanding, prediction, and control) but the methods are different Requires different frameworks and methodologies which are not as well developed as experimental reductionism Mathematical simulations Complex statistical modeling Nonlinear models Multilevel models Evaluation of real-world interventions It becomes difficult to make reassuring cause and effect statements; Scientists are forced to live with uncertainty. It becomes difficult to create unambiguous mechanistic explanations
Example: Obesity Epidemic The United States and other developed countries are experiencing an epidemic of obesity Why is this happening? What can be done to reverse the trends? Problem is so serious that life expectancies may begin to decline by the middle of the 21 st century
Obesity Trends* Among U. S. Adults BRFSS, 1985 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1986 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1987 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1988 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1989 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1990 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1991 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1992 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1993 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1994 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1995 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1996 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC.
Obesity Trends* Among U. S. Adults BRFSS, 1997 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. ≥ 20%
Obesity Trends* Among U. S. Adults BRFSS, 1998 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. ≥ 20%
Obesity Trends* Among U. S. Adults BRFSS, 1999 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. ≥ 20%
Obesity Trends* Among U. S. Adults BRFSS, 2000 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. ≥ 20%
Obesity Trends* Among U. S. Adults BRFSS, 2001 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% ≥ 25%
Obesity Trends* Among U. S. Adults BRFSS, 2002 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% ≥ 25%
Obesity Trends* Among U. S. Adults BRFSS, 2003 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% ≥ 25%
Obesity Trends* Among U. S. Adults BRFSS, 2004 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% ≥ 25%
Obesity Trends* Among U. S. Adults BRFSS, 2005 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
Obesity Trends* Among U. S. Adults BRFSS, 2006 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
Obesity Trends* Among U. S. Adults BRFSS, 2007 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
Obesity Trends* Among U. S. Adults BRFSS, 2008 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
Obesity Trends* Among U. S. Adults BRFSS, 2009 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
Obesity Trends* Among U. S. Adults BRFSS, 2010 (*BMI ≥ 30, or ~ 30 lbs. overweight for 5’ 4” person) No Data <10% 29% ≥ 30% 10%– 14% 15%– 19% Source: Behavioral Risk Factor Surveillance System, CDC. 20%– 24% 25%–
How can we explain this? What are some possible explanations? Is there a single cause we need to be looking for? If there are multiple causes, how do we study them? Are the causes additive or synergistic? Do the causes cascade across levels of analysis (e. g. , macroeconomic factors influencing individual behaviors)? Does our framework (reductionism versus complex systems science) make a difference in how we approach these problems?
Reflections The question is not which approach is the best approach, but which is the best for solving a specific problem Reductionism does not automatically lead to translation research Complex systems science may have much more translation potential Complex systems science requires interdisciplinary research, different methodological approaches, and the abandonment of simple one-cause explanations
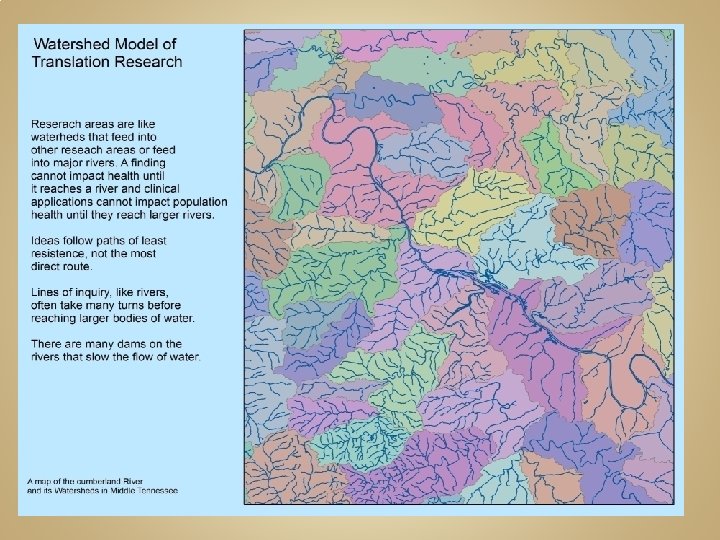
What characterizes “translation” research? Addresses problems in clinical care and population health Evidence-based (based on best science available) Involves transfer of knowledge and or methods across disciplinary boundaries Requires consideration of context (target is imbedded in real-world systems) Coalitions and partnerships Engagement of communities Moves away from trying to find a single causal factor and towards
Familiar example of complex systems approach to improve chronic disease management
Challenges Personalized medicine? Matching drugs to genes How about matching treatment to other systems that are influencing health Family Neighborhood Work setting Psychology (cognition and emotion) Health services research? Are there gains to be had from adopting complex systems framework? Need viable alternatives to the clinical trial Implementation science? Can methods such as continuous quality improvement become scientific tools for answering questions about improving clinical care and population health What other methods can be adapted?