Rastreamento de Cncer de Mama Uma homenagem ao




")
 • FALTA DE ATIVIDADE")





: 1685 -1692.")

: 1685 -1692.")





- Slides: 26
Rastreamento de Câncer de Mama Uma homenagem ao Outubro Rosa
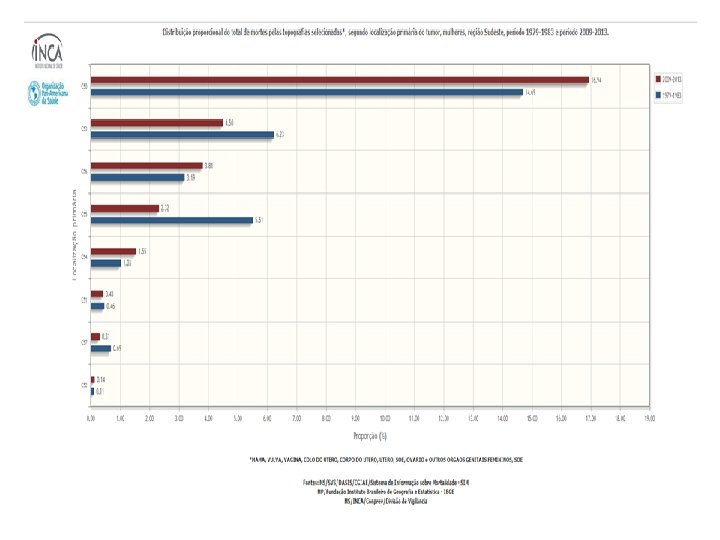
Como se distribui o diagnóstico e a morte por câncer? • Os mais ricos OU os mais pobres. . . • têm mais (diagnóstico de) câncer (incidência) • e morrem mais daquele câncer (mortalidade específica)? • ou morrem mais (mortalidade geral)? • DEPENDE DO C NCER • Se sim, porque? “Sobrediagnóstico” • Overdiagnosis é um diagnóstico verdadeiro, porém desnecessário, com maior potencial de causar danos do que benefícios. Este fenômeno decorre da cultura do check-up, propagada pelo lobby em prol do excesso de exames em pessoas saudáveis.
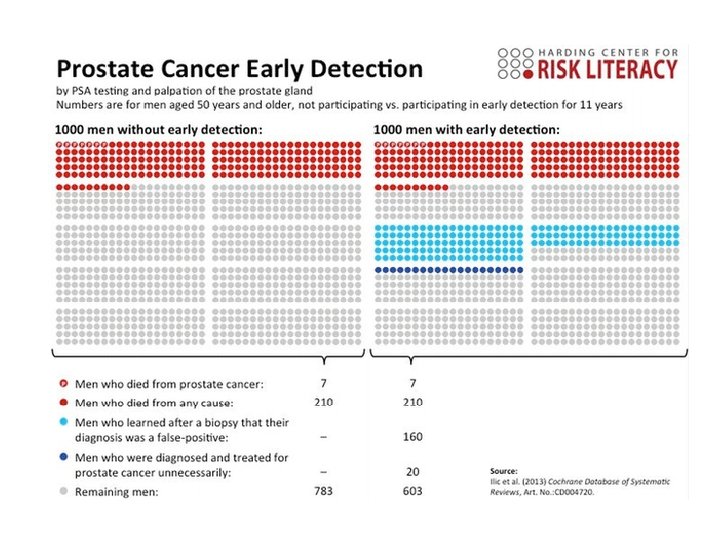
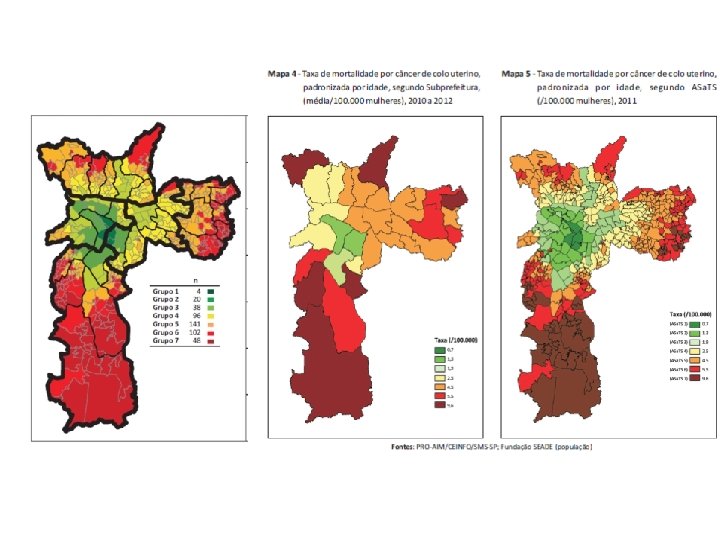
Como se distribui espacialmente o diagnóstico e a morte por câncer? • Rastreamento seguro e efetivo -> reduz morbidade e mortalidade • Ex. papanicolaou (citologia oncótica do colo do útero) • Rastreamento inseguro e inefetivo -> pode aumentar a morbidade e mortalidade (geral e específica) • Ex. de rastreamentos questionáveis: mamografia e PSA (câncer de próstata)
Modelos explicativos sobre câncer de mama – incidência e mortalidade O problema do lead time bias (viés do tempo de espera) e a invisibilidade dos efeitos adversos
O que as mulheres imaginam de proteção (entendem que os médicos dizem)
FATORES DE RISCO “AMBIENTAIS E DE ESTILO DE VIDA" (MODIFICÁVEIS) • FALTA DE ATIVIDADE FÍSICA • ESTAR ACIMA DO PESO OU OBESO • DIETA POBRE EM ALIMENTOS NÃOPROCESSADOS • TERAPIA DE REPOSIÇÃO HORMONAL COMBINADA (HRT): TOMAR A TERAPIA DE REPOSIÇÃO HORMONAL COMBINADA PARA A MENOPAUSA, PODE AUMENTAR O RISCO DE C NCER DE MAMA E AUMENTA O RISCO DE QUE O C NCER SERÁ DETECTADO EM UM ESTÁGIO MAIS AVANÇADO. • CONSUMO DE BEBIDAS ALCOÓLICAS QUANTO MAIS ÁLCOOL QUE VOCÊ CONSOME, MAIOR O RISCO. • RADIAÇÃO NO PEITO: TENDO A TERAPIA DE RADIAÇÃO PARA O PEITO ANTES DA IDADE DE 30 PODE AUMENTAR O RISCO DE C NCER DE MAMA. http: //www. nationalbreastcancer. org/breast-cancer-risk-factors
http: //www. yourdiseaserisk. wustl. edu/Common. Pdf/Relative. Risks. pdf
Loberg M, Lousdal ML, Bretthauer M, Kalager M. Benefits and harms of mammography screening. Breast Cancer Research. 2015, 17: 63.
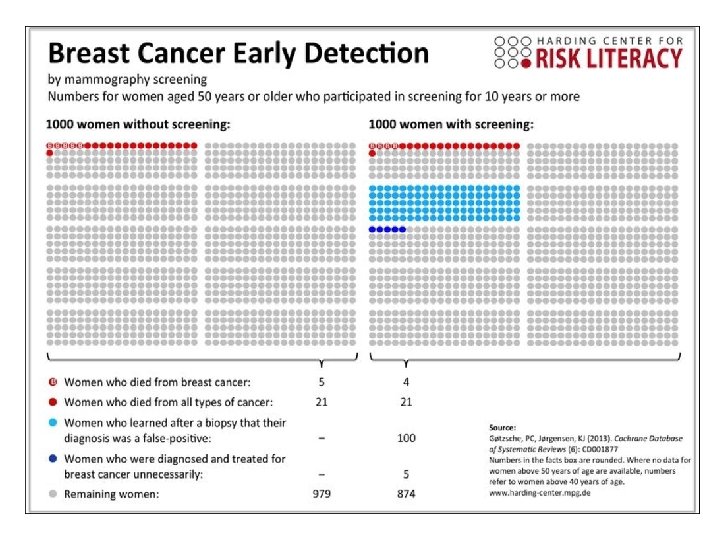
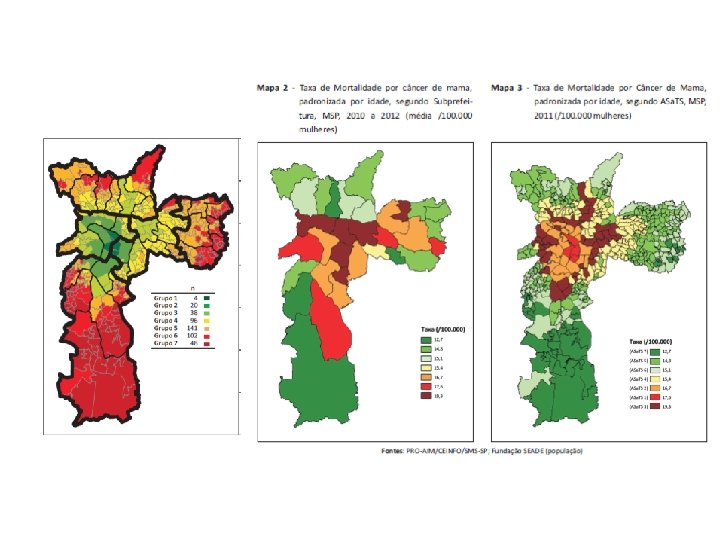
O que eu nós achávamos, até julho: • A mamografia não reduzia a mortalidade geral, no máximo reduzia minimamente, e talvez, a mortalidade específica por câncer de mama. • Além de causar problemas graves de sobrediagnóstico e sobretratamento, que são agora considerados agravos à saúde. O que nós descobrimos: • Saíram vários estudos grandes dizendo que a mamografia não reduz nem mesmo a mortalidade por câncer de mama, • não reduz os casos avançados como se acreditava, nem reduz o número de cirurgias mutiladoras. • Enfim, parece que ficamos só com os danos. • Isso talvez ajude a explicar porque este resultado encontrado por vocês de quanto mais mamografia, mais morte. • Mais ricas e mais escolarizadas, mais setor suplementar, mais TRH e mais mamografias, mais incidência e mais morte
O viés de publicação – caso do TRH e câncer de ovário Figure 2. Relative risk of ovarian cancer by duration of use in current and past users of hormone therapy*Risk relative to never-users of hormone therapy, stratified by age at diagnosis, study, and body-mass index, and adjusted for age at menopause, hysterecto. . . Collaborative Group on Epidemiological Studies of Ovarian Cancer Menopausal hormone use and ovarian cancer risk: individual participant meta-analysis of 52 epidemiological studies null, Volume 385, Issue 9980, 2015, 1835– 1842 http: //dx. doi. org/10. 1016/S 0140 -6736(14)61687 -1
From: Rethinking Screening for Breast Cancer and Prostate Cancer JAMA. 2009; 302(15): 1685 -1692. doi: 10. 1001/jama. 2009. 1498 Figure Legend: Three hypothetical scenarios of changes over time in stage-specific incidence rates associated with widespread screening usage are presented. The dotted lines indicate the point of screening initiation. The fraction of localized and regional disease before and after screening is shown for each scenario A, Screening leads to an increase in localized cancers, a decrease in regional cancers, and stable rates of overall invasive cancer (after an initial increase following introduction of screening). B, Screening leads to an increase in the detection of total and early stage cancers but without a decrease in the rate of regional cancers. C, Screening results in an increase in early and overall cancer rates, with some decrease in regional stage disease. This outcome is intermediate between A and B. D, The incidence of localized and regional cancers is shown for the prescreening period and for each of the scenarios. The height of the bars represents total incidence. E, The relative percentage of localized vs regional cancers is shown. Note that all 3 scenarios lead to the same increase in the percentage of detection of localized cancers. Date of download: 10/14/2015 Copyright © 2015 American Medical Association. All rights reserved.
Câncer de mama e de próstata, impacto do rastreamento sobre a incidência
From: Rethinking Screening for Breast Cancer and Prostate Cancer JAMA. 2009; 302(15): 1685 -1692. doi: 10. 1001/jama. 2009. 1498 Figure Legend: A, Age-adjusted incidence rate by stage of invasive female breast cancers for all ages, SEER 1973 -2006. Mammography was introduced in 1983 and more widely used beginning in 1986. The incidence per 100 000 women of localized, regional, and metastatic breast cancer is shown over time (left), and for the period prior to the uptake of screening (1982) and 16 years after (1998) (middle). Local disease, as a fraction of all cancers reported, is shown on the right. B, Age-adjusted incidence rate of adenocarcinoma of the prostate for men older than 24 years, SEER, 1973 -2006. Prostate cancer screening began in 1986 and was more widely used beginning in 1989 -1990. Given the degree of missing data for prostate cancer TNM stage in SEER, we chose to show the change in Gleason grade, a significant predictor of outcome since the introduction of screening. The middle panel shows the incidence per 100 000 men of tumors with Gleason grades that were low- and intermediate-grade (2 -7) vs high-grade (8 -10) tumors, for the period prior to the uptake of screening (1988) and 16 years after (2004). The low- and intermediate-grade tumors as a fraction of all cancers is shown in the panel on the right. Date of download: 10/14/2015 Copyright © 2015 American Medical Association. All rights reserved.
Use of Screening Mammography and Incidence of Stage. Specific Breast Cancer in the United States, 1976– 2008. Bleyer A, Welch HG. N Engl J Med 2012; 367: 1998 -2005.
O que reduz a incidência de late stage?
Trends in the Annual Incidence of Late-Stage Breast Cancer and Its Two Components (Regional and Distant Disease) among U. S. Women 40 Years of Age or Older, 1976– 2008. Bleyer A, Welch HG. N Engl J Med 2012; 367: 1998 -2005.
A mortalidade por câncer de mama em SP aumentou ano a ano: 12, 72/100. 000 em 2009; 13, 18 em 2010; 13, 36 em 2011; 13, 45 em 2012; 14, 02 em 2013