Peripheral nerve Entrapments DR Eslam Elsayed Lecturer of










 ØIt is the most common entrapment neuropathy. ØIt is the")















 ØULNAR TUNNEL SYNDROME (GUYON’S CANAL")








: Simple decompression by spliting covering fascia. Medial humeral epicondylectomy. Anterior")


- Slides: 44
Peripheral nerve Entrapments DR. Eslam El-sayed Lecturer of neurosurgery S. V. U
OBJECTIVES l Anatomical review. l entrapment sites. l Basics for entrapment l Examples of nerve entrapment l Special test (motor and sensory) l management
NUMBER OF THE PERIPHERAL NERVES IN THE HUMAN BODY ? ?
Examples of entrapment neuropathy l Median nerve entrapment: l Ulnar nerve entrapment: l Radial nerve entrapment:
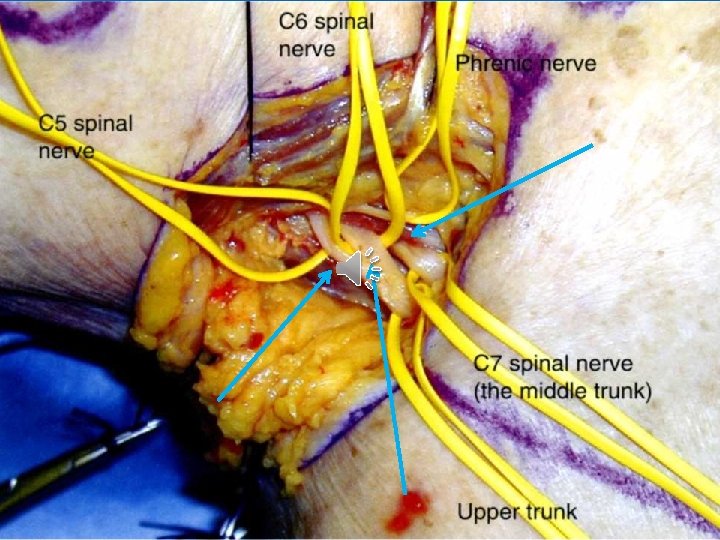
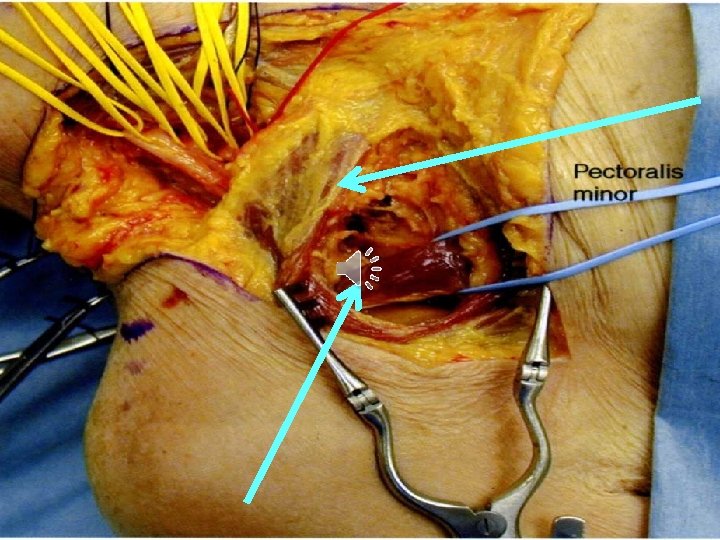
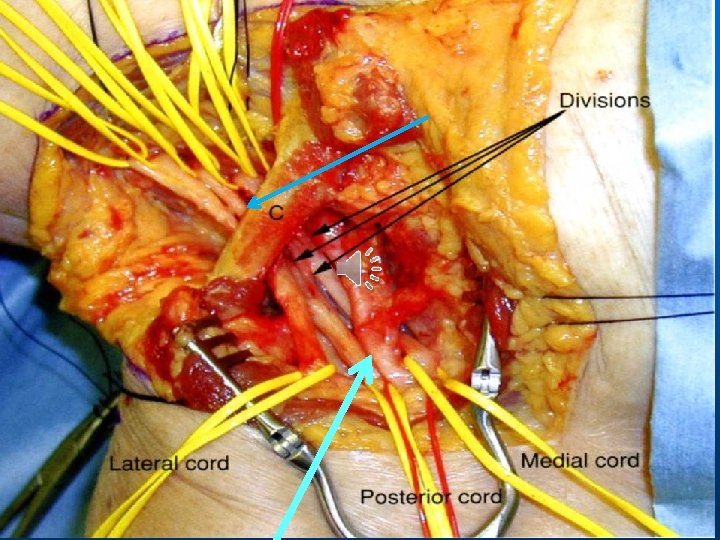
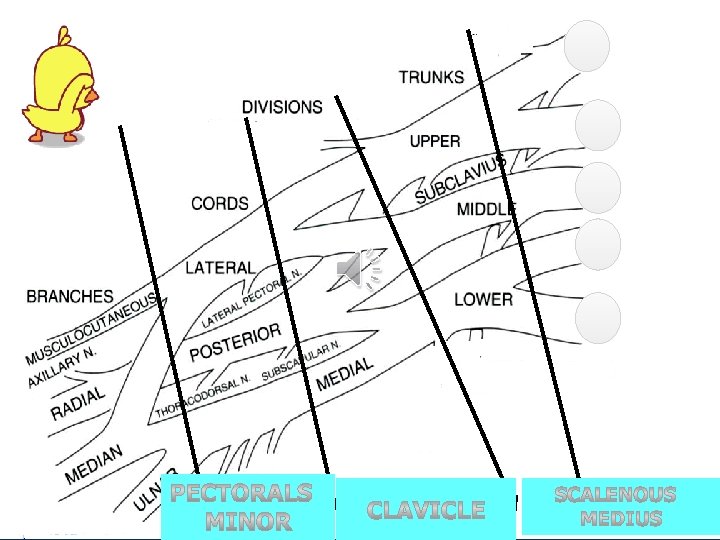
Anatomy Median nerve C 5 -T 1
Anatomy Median nerve C 5 -T 1
Anatomy Median nerve C 5 -T 1
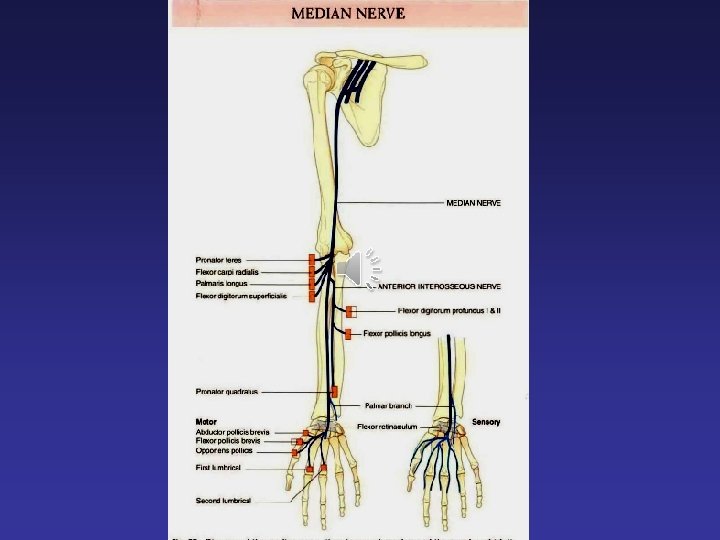
Median nerve - Entrapment Sites of the median nerve compression : I- At the elbow and forearm (high median nerve palsy): 4 sites 1. By the Ligament Of Struthers in the distal humerus at the elbow (LS in the figure). 2. By the thickening of the Bicipital Aponeurosis in the elbow. Also known as lacertus fibrosus, 3. Between the two heads of pronator tears pronator teres syndrome (PTS ). 4. By the thickening of the flexor digitorum superficalis in the proximal forearm (FDS) II- At the wrist, 1. carpal tunnel syndrome 2. Deep branch of the median nerve
DEFENITION
Carpal tunnel syndrome (CTS) ØIt is the most common entrapment neuropathy. ØIt is the commonest OCCUPATIONAL disease affecting the peripheral nerves. Ø 90% of all entrapment neuropathies.
ANATOMY Boundaries of the tunnel: the CT lies distal to the wrist crease Roof: TCL (flexor retinaculum)
ETIOLOGY
A. Local causes l Inflammatory: e. g. tenosynovitis, histoplasma fungal infection, hypertrophic synovium l Trauma: e. g. Colles’ fracture, dislocation of one of the carpal bones l Tumors: e. g. Haemangioma, cyst, ganglion, lipoma, neuroma etc. l Anatomical anomalies: e. g. thickened transverse carpal ligament, bony abnormalities, abnormal muscle bellies, persistent median artery etc. C. Systemic causes B. Regional causes l Osteoarthritis l Rheumatoid arthritis l Amyloidosis l Gout l l l l • Diabetes • Obesity • Hypothyroidism • Pregnancy • Menopause • Systemic lupus erythematosus • Scleroderma • Dermatomyositis • Renal failure • Long-term haemodialysis • Acromegaly • Multiple myeloma • Sarcoidosis • Leukemia • Alcoholism • Hemophilia
l Symptoms • A tingling or numb feeling in the hand and/or fingers specially at night. • Shooting pains in the wrist or forearm, and sometimes extending to the shoulder, neck • Difficulty clenching the fist or grasping small objects;
Signs l Tinel sign l Phalen's test
Diagnosis of Nerve Entrapment – Clinical examination • Brief limb survey for detection of local causes • Screening sensation test – Light touch of affected area compared to known normal • Two point discrimination – Can remain normal if minimal number of fibers functioning normally l Sensory threshold tests, such as Semmes-Weinstein monofilament test or those measuring vibration sensitivity. These are the most sensitive tests for the detection of early and slight neurological dysfunction
Motor examination The ulnar nerve innervate all the muscle of the hand except 5 muscles v 3 pollicies (abductor brevis, flexor brevis and opponce) v 2 lumbricals (index and middle finger)
Diagnosis of Nerve Entrapment – Electro diagnostic studies • Diagnostic gold standard • Can aid in confirming diagnosis in some cases • Fallible to user error and sensitivity of equipment
Diagnosis of Nerve Entrapment – Radiographic examination • Occasionally useful • Rule out neck pathology in diffuse presentation • C-xray – Pancoast tumor • US: • MRI – Best study for showing nerve compression at brachial plexus down to carpal tunnel
Treatment
Brace
Injection
Open surgery
Øcubital tunnel syndrome TARDY ULNAR NEURITIS (SULCUS ULNARIS SYNDROME) ØULNAR TUNNEL SYNDROME (GUYON’S CANAL SYNDROME). ØSYNDROME OF DEEP BRANCH ENTRAPMENT OF THE ULNAR NERVE. (LESS COMMON) 1
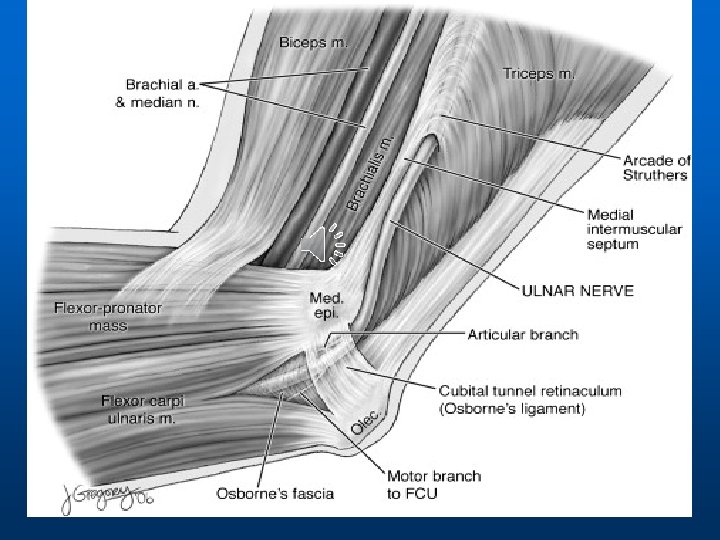
cubital tunnel syndrome Compression of the ulnar nerve in the cubital tunnel in the posterior surface of the medial humeral epicondyle also called Tardy ulnar neuritis.
cubital tunnel syndrome 1 2 2
ETIOLOGY
CLINICAL SYMPTOMS AND SIGNS – Paresthesias, numbness and pain develop in the small , ringer fingers and the ulnar side of the palm.
• Decreased 2 point discrimination Elbow flexion-pressure test: Weakness in FDP of the small finger and FCU Froment’s sign • Claw hand MP hyperextension • • •
�Late stages atrophy & Muscle wasting �Loss of ulnar innervation will lead to a claw-hand appearance.
q. Electromyography and nerve conduction velocity. Motor conduction velocity across the elbow is useful to define management: < 40 m/second propably indicates surgical intervention. q. High-resolution ultrasonography. The ultrasonography measurement of the cross-sectional area of the ulnar nerve. q. Radiographic studies allow visualization of rheumatic, arthritic, or posttraumatic changes around the elbow.
TREATMENT Conservative therapy § Splints prevents elbow extension try to prevent repetitive nerve irritation. § The sulcus may be injected into the center of an imaginary line connecting the medial epicondyle to the median edge of the olecranon.
Cubital tunnel syndrome approaches(options): Simple decompression by spliting covering fascia. Medial humeral epicondylectomy. Anterior subcutaneous transposition of the U. N. Anterior submuscular transposition. Intramuscular transposition.
Outcome • Minimal compression –Excellent results in 90% • Moderate compression –Excellent in 50%
l Thank you