Melanoma By Dr Abeer Elsayed Aly Lecturer of

Melanoma By Dr Abeer Elsayed Aly Lecturer of medical oncology SECI 19/03/2013
 – 59, 580 new cases • 33,")
Melanoma Incidence and Mortality • Incidence (US) – 59, 580 new cases • 33, 580 new male cases • 26, 000 new female cases • 12 per 100, 000 population • Mortality (US) – 7, 770 total • 4, 910 males • 2, 860 females American Cancer Society, Cancer Facts and Figures. 2005.

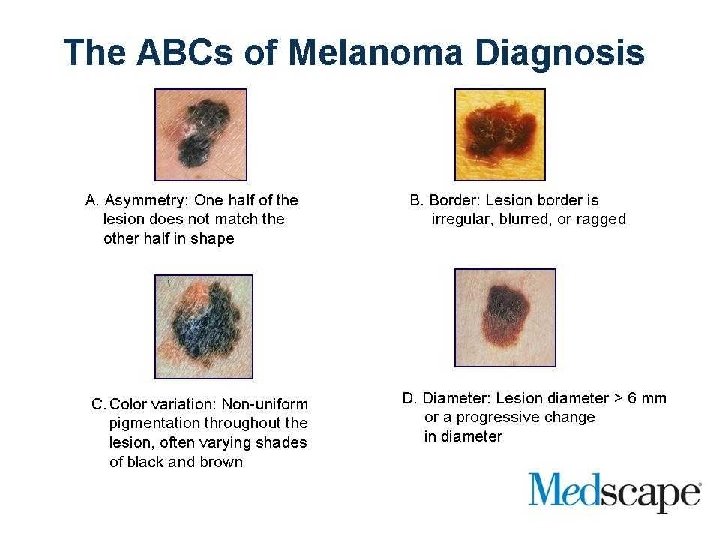
Melanoma: risk factors • Constitutional predisposition – Fair skin/hair color/ freckling – Burn vs tan – >20 benign nevi (moles) or >3 atypical nevi – Family history of dysplastic nevi – Increasing age – Immunosuppression – Xeroderma pigmentosum – H/O solar keratosis, squamous cell carcinoma

Melanoma: risk factors • Risk behaviors – >3 sunburns – Episodic excessive sunlight exposure – Long term continuous sunlight exposure – UV exposure at tanning salons
: – Early detection – Rapid growth/high proliferation rate – Chemotherapy")
Melanoma The challenge (historically): – Early detection – Rapid growth/high proliferation rate – Chemotherapy resistant – Radiation resistant – Short anticipated survival

Types of Melanoma • • • Acral lentiginous Mucosal melanoma Superfical spreading melanoma Lentigo maligna melanoma Nodular melanoma

Superficial spreading • most common head and neck, 50% • 4 th to 5 th decade • clinical mixture of brown/tan, pink/white irregular borders, biphasic growth • irregular nests in epidermis • underlying lymphoid infiltrate • enlarged nests and single cells in all epidermal layers

Lentigo maligna • • • 20% of head and neck longest radial growth phase >15 yrs elderly sun exposed areas clinical dark, irregular ink spot contiguous lintiginous proliferation, dyshesive, variable shape, atrophic epidermis, infundibular basal cell layer of hair follicles

Lentigo maligna

Nodular melanoma 30% of head and neck 5 th decade aggressive monophasic growth sun-exposed and nonexposed areas well circumscribed blue/black or nodular with involution in irregular plaque • downward tumorigenic growth, expand papillary dermis into reticular dermis • • •

Nodular melanoma

Mucosal melanoma • • • 8% head and neck histologic staging little use local control predicts survival neck dissection for clinical N+ XRT for histo N+ adjuvant interferon alpha 2 -b

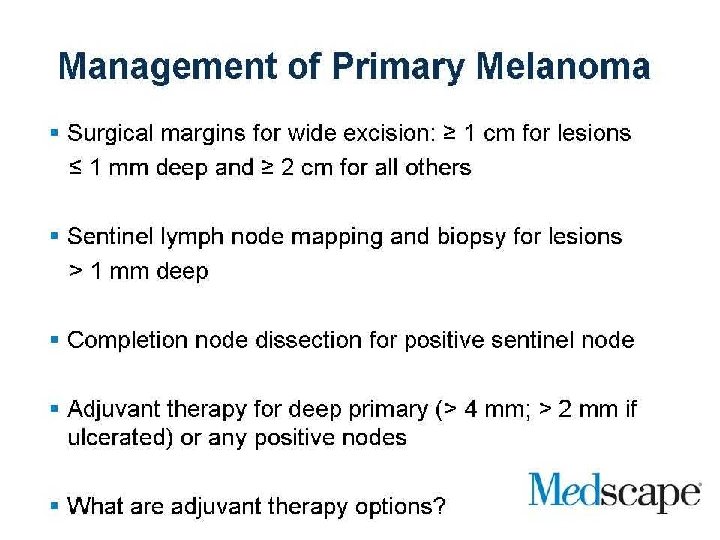
Biopsy techniques • Excisional biopsy 1 -3 mm margins avoid wider margins (accurate lymphatic mapping) • Full thickness incisional/punch biopsy for large lesions of the palms, soles, digits, face, ears • Deep shave biopsies When suspicion for melanoma is low NCCN Guidelines 2005

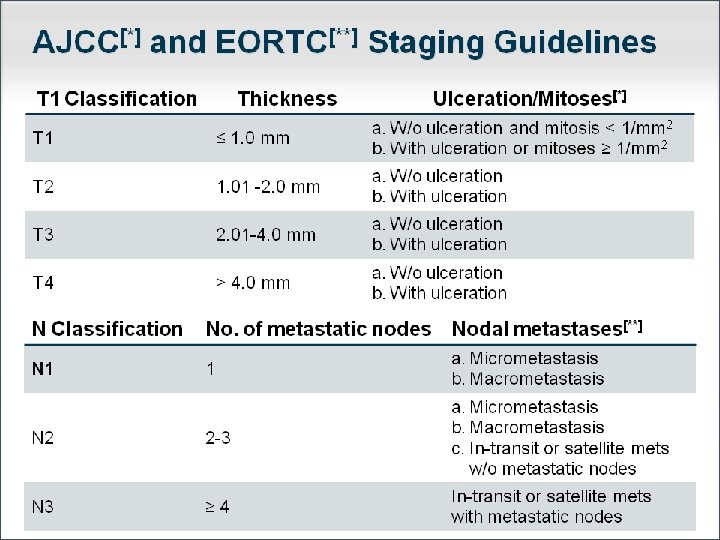
Staging system

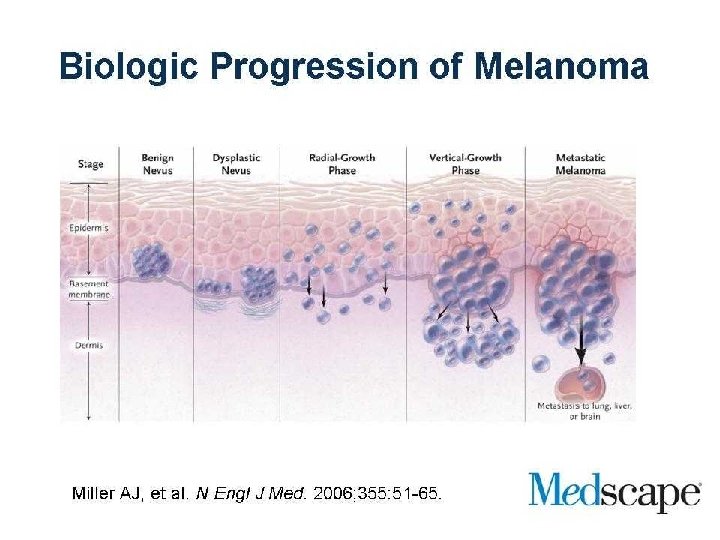
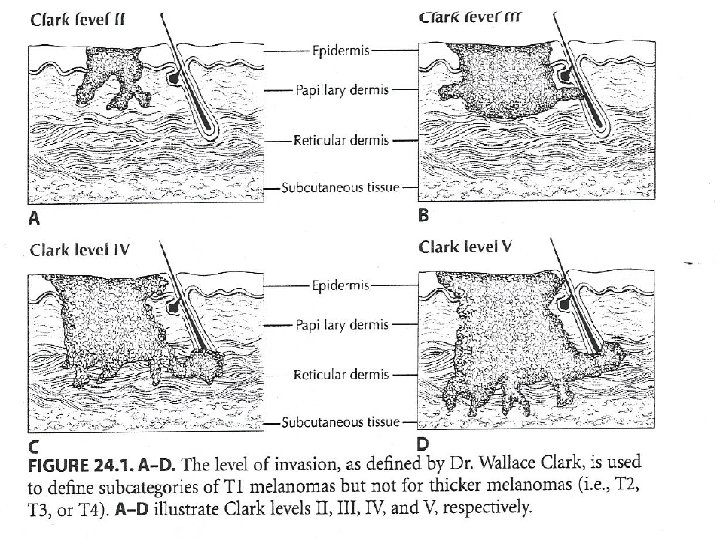
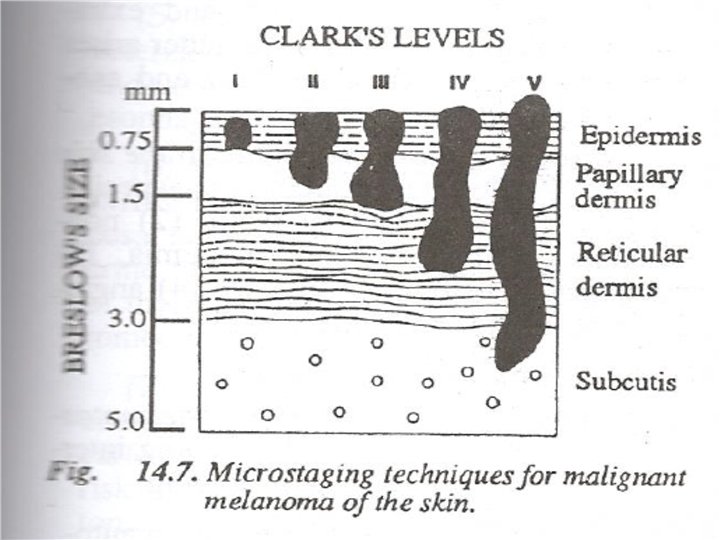
Clark staging • Based upon histologic level of invasion • Level I – Epidermis only (in situ) • Level II – Invades the papillary dermis, but not to the papillary-reticular interface • Level III – Invades to the papillary-reticular interface, but not into the reticular dermis • Level IV – Into the reticular dermis • Level V – Into subcutaneous tissue

Breslow staging • • • Based upon absolute depth of invasion Stage I – < 0. 75 mm Stage II – 0. 76 – 1. 5 mm Stage III – 1. 51 – 4. 0 mm Stage IV - > 4. 0 mm

Work up • Labs – LDH • Radiology – – CXR Possible CT for metastasis Possible CT abdomen, MRI brain Possible Lymphoscintigraphy • Excision – 2 cm margins • Adjunctive Therapy – Possible elective neck dissection – Possible sentinel lymph node biopsy – Possible elective radiation
 Nodal status Ulceration Mitosis Satellite lesions")
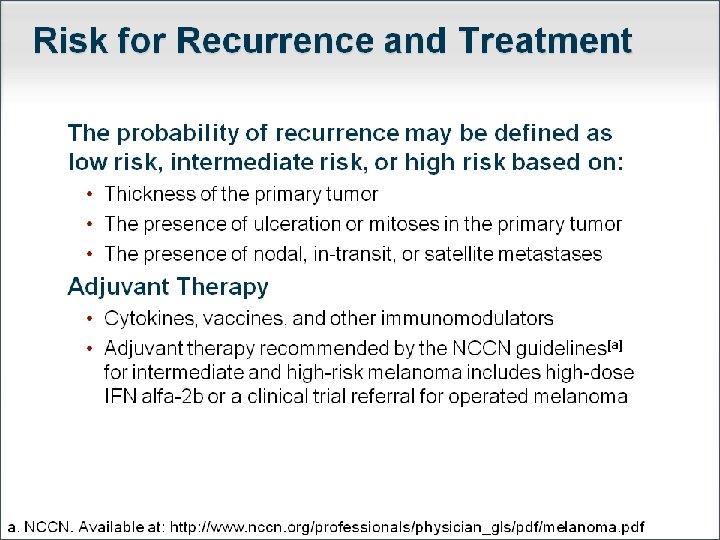
Prognostic indicators • • • Thickness (Breslow depth) Nodal status Ulceration Mitosis Satellite lesions In transit lesions
 Nodal status Ulceration Mitosis Satellite lesions")
Prognostic indicators • • • Thickness (Breslow depth) Nodal status Ulceration Mitosis Satellite lesions In transit lesions
 Nodal status Ulceration Mitosis Satellite lesions")
Prognostic indicators • • • Thickness (Breslow depth) Nodal status Ulceration Mitosis Satellite lesions In transit lesions

Prognostic Indicators: Nodal status • OS for patients with 1 positive sentinel node is 60% at 5 years • OS for patients with a single palpable node is 40% at 5 years • Gershenwald et al, 2001
 Nodal status Ulceration Mitosis Satellite lesions")
Prognostic indicators • • • Thickness (Breslow depth) Nodal status Ulceration Mitosis Satellite lesions In transit lesions

Mitotic Index • N = 3661 from the Sydney Melanoma Database • Correlated – – clinical information (survival) primary tumor thickness (Breslow depth) ulcerative state (infiltrative, attenuative, and traumatic) tumor mitotic rate (TMR) (at the invading front, deep border) • Conclusion: TMR is a more powerful prognostic indicator than ulceration in patients with primary cutaneous melanoma Azzola et al, Cancer 2003
 Nodal status Ulceration Mitosis Satellite lesions")
Prognostic indicators • • • Thickness (Breslow depth) Nodal status Ulceration Mitosis Satellite lesions In transit lesions

Risk of In-Transit Metastasis • In- transit metastasis – Cutaneous / subcutaneous tissue – Between the primary tumor – and the draining lymph node basin • 5 yr survival rates: 12% - 37% • Risk factors: – Thicker primary – Lower extremity – Regional LN metastasis

Other prognostic factors: • LDH – Elevated levels correlate with: Early recurrence Shorter survival (Newcki et al, 2008) • Serum S 100 level – Early studies suggest: Shorter survival Early distant relapse Poorer response to treatment • Microvessel Density (Smith et al, 2008)

Other prognostic factors: • LDH – Elevated levels correlate with: Early recurrence Shorter survival (Newcki et al, 2008) • Serum S 100 level – Early studies suggest: Shorter survival Early distant relapse Poorer response to treatment • Microvessel Density (Smith et al, 2008)

Other prognostic factors: – Elevated levels correlate with: Early recurrence Shorter survival LDH • (Newcki et al, 2008) • Serum S 100 level – Early studies suggest: Shorter survival Early distant relapse Poorer response to treatment • Microvessel Density (Smith et al, 2008)
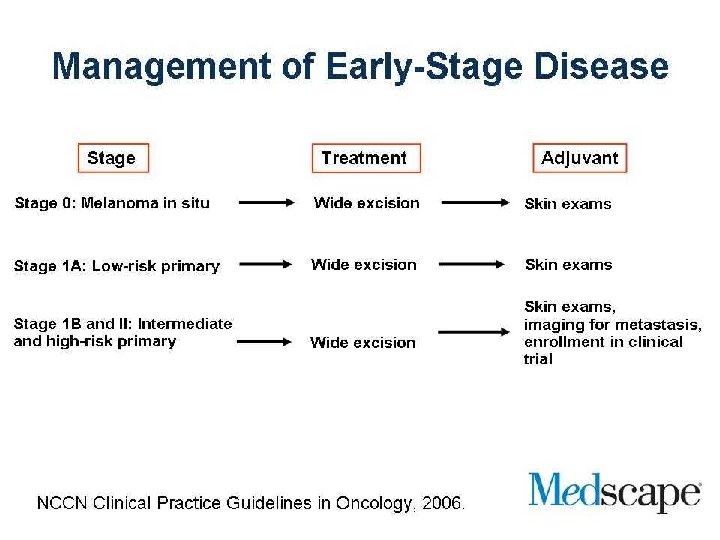
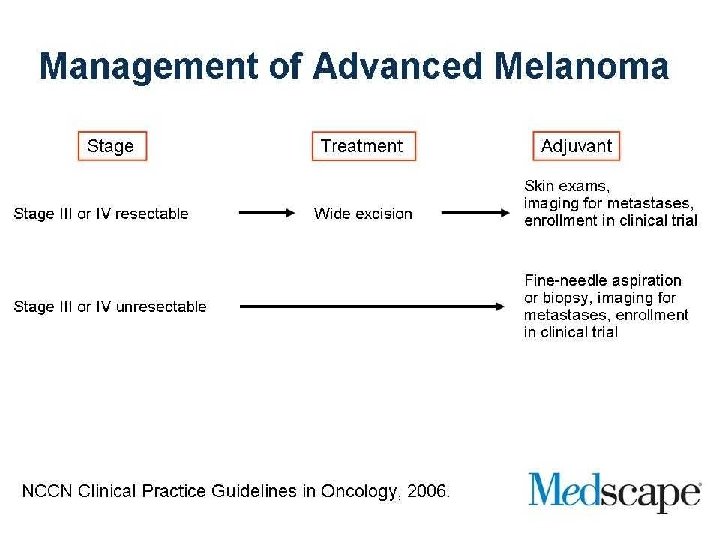

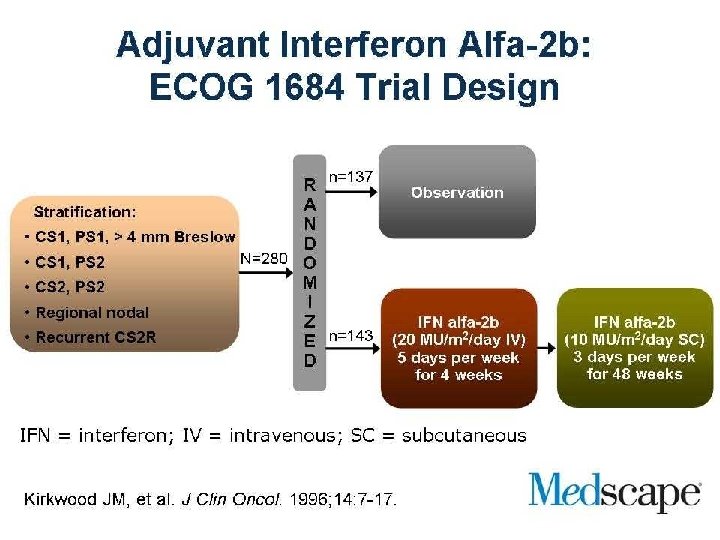
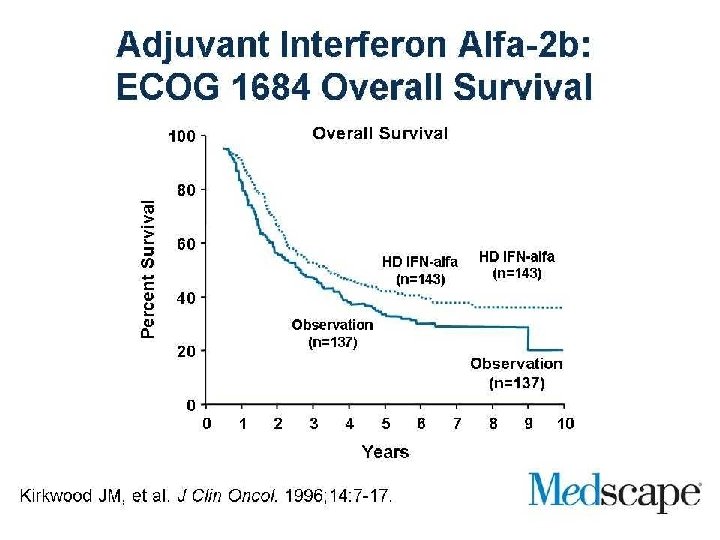
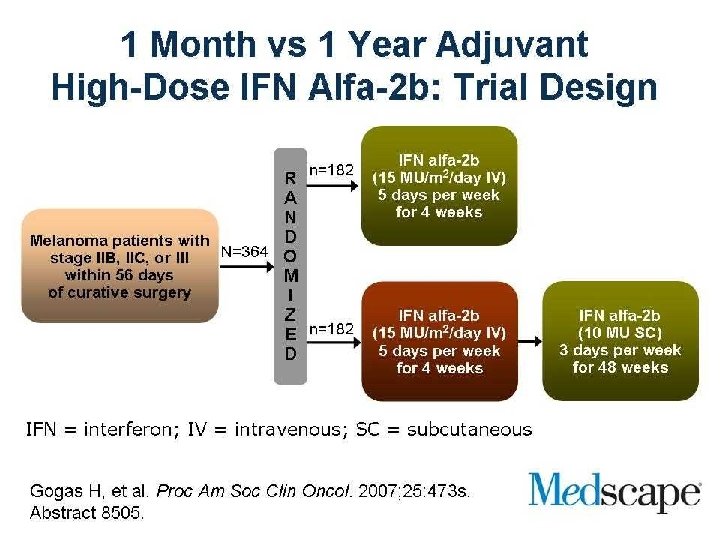
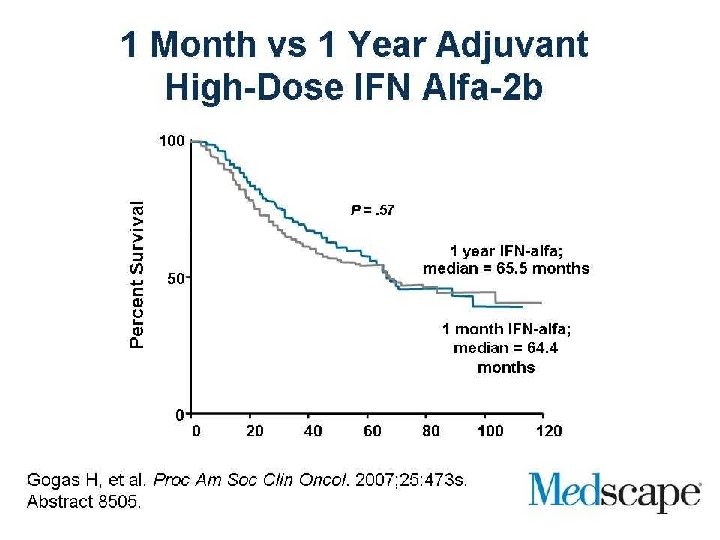
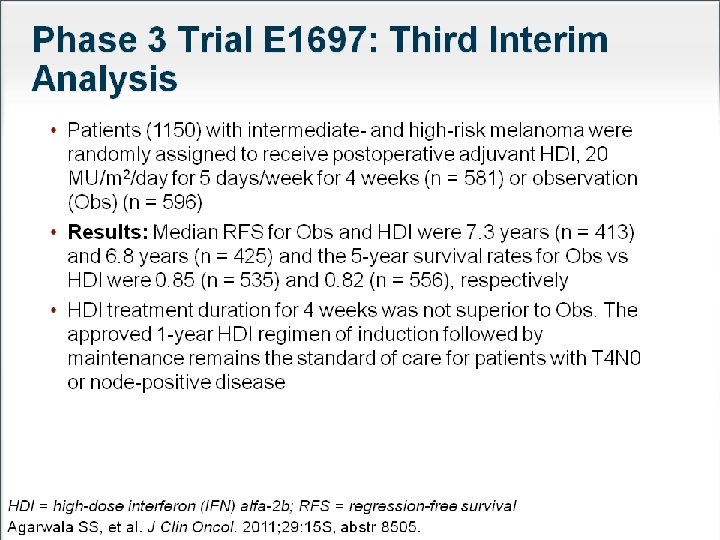
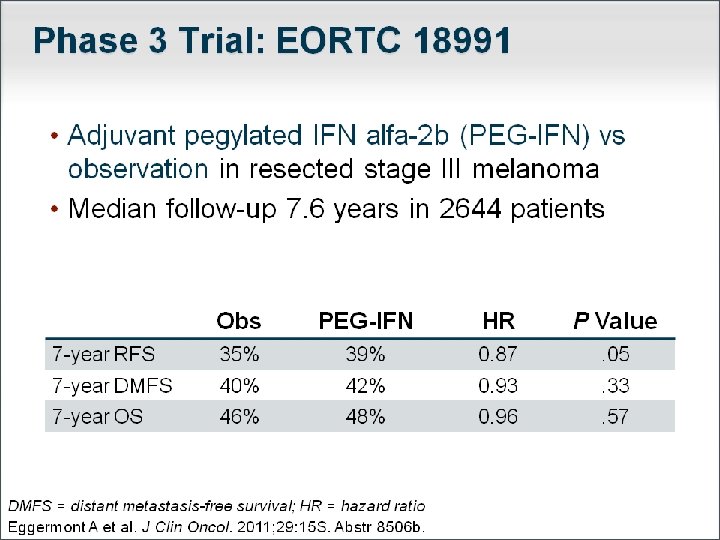
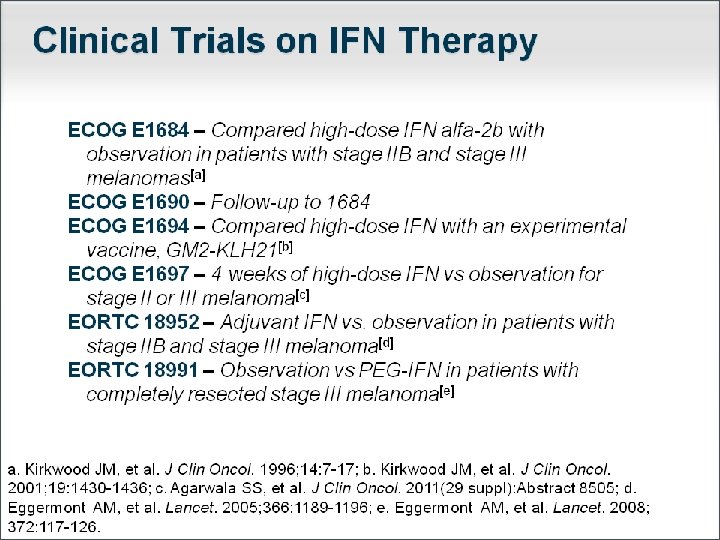
Adjuvant treatment
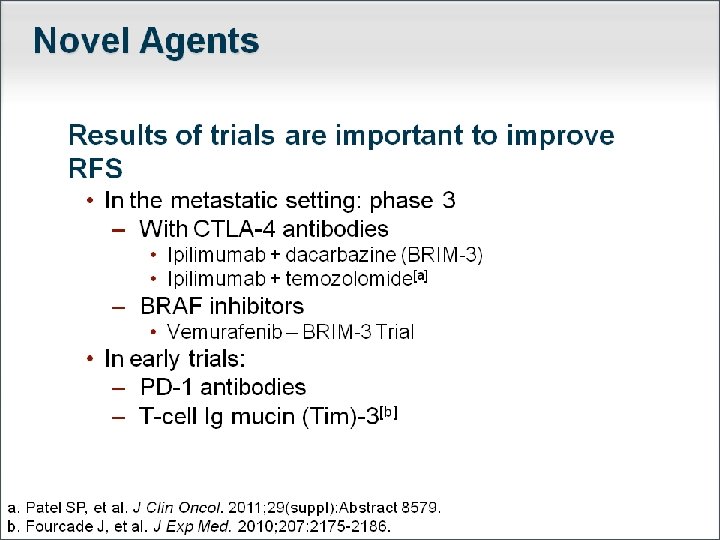

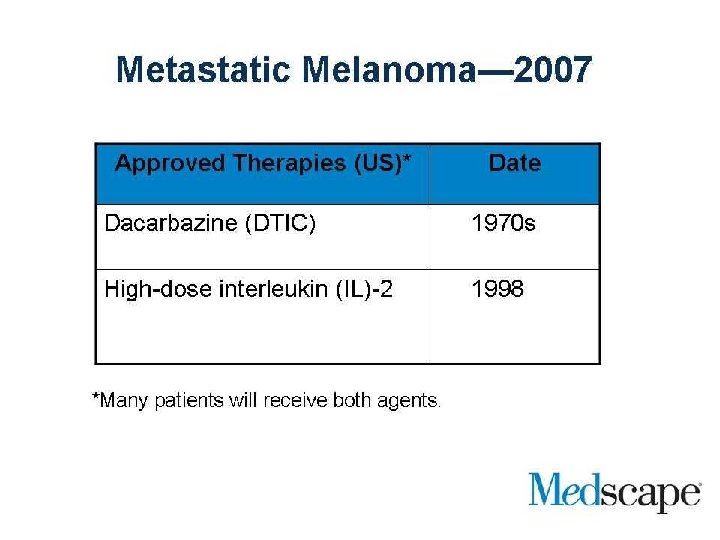
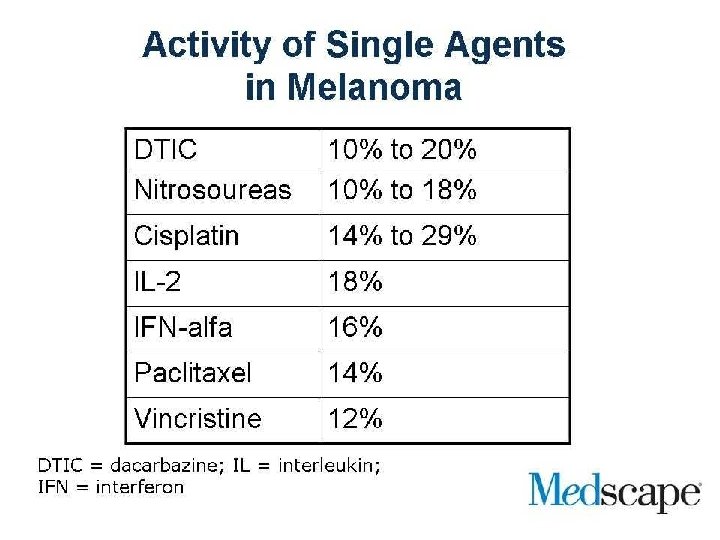
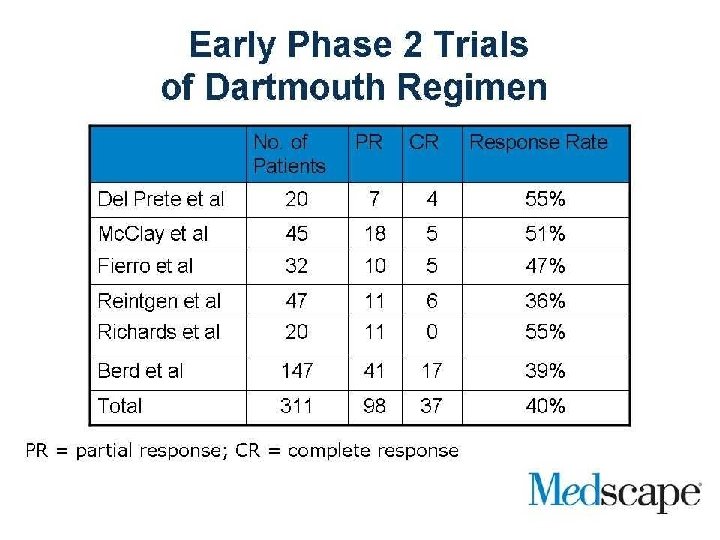
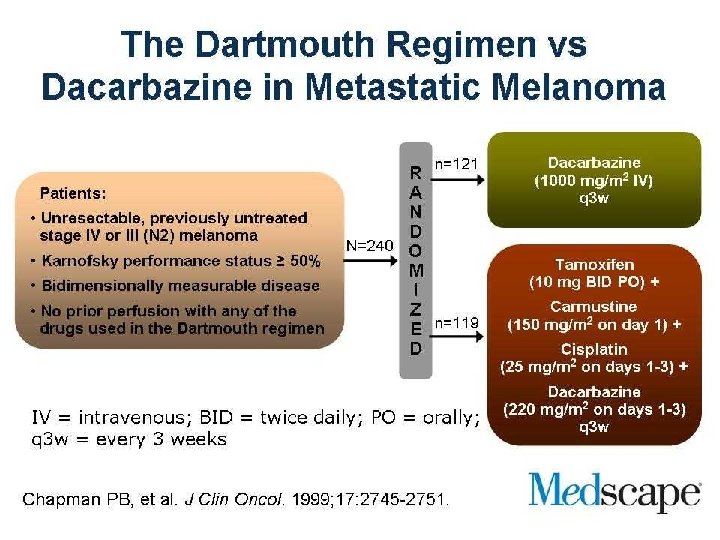
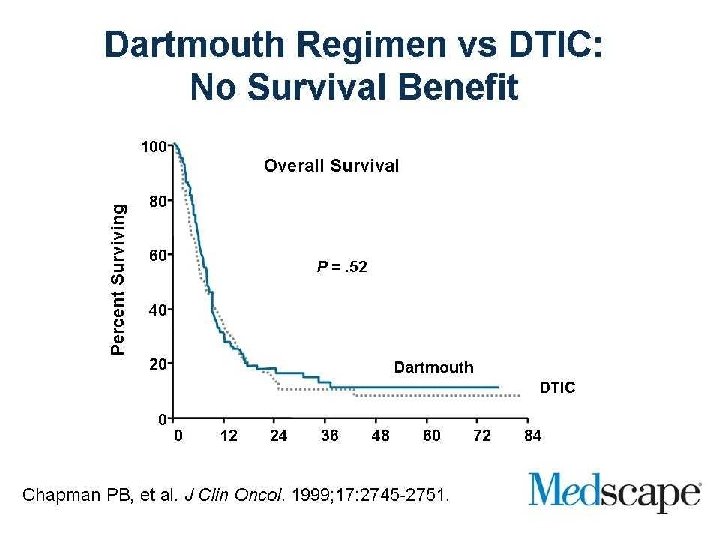
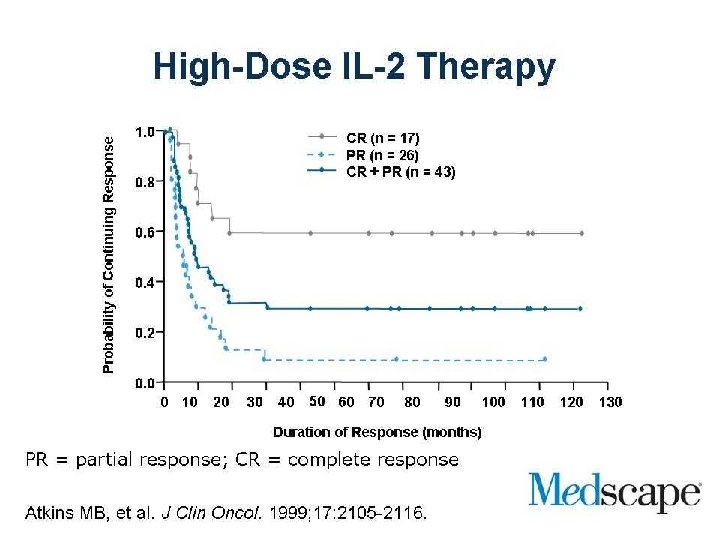
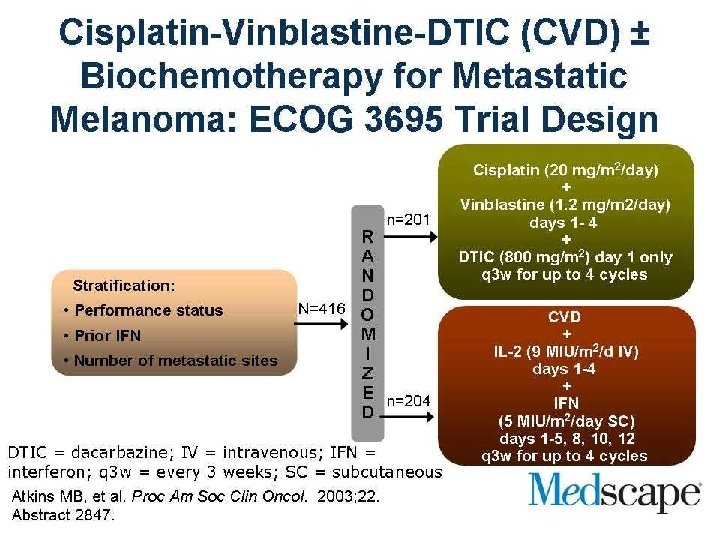
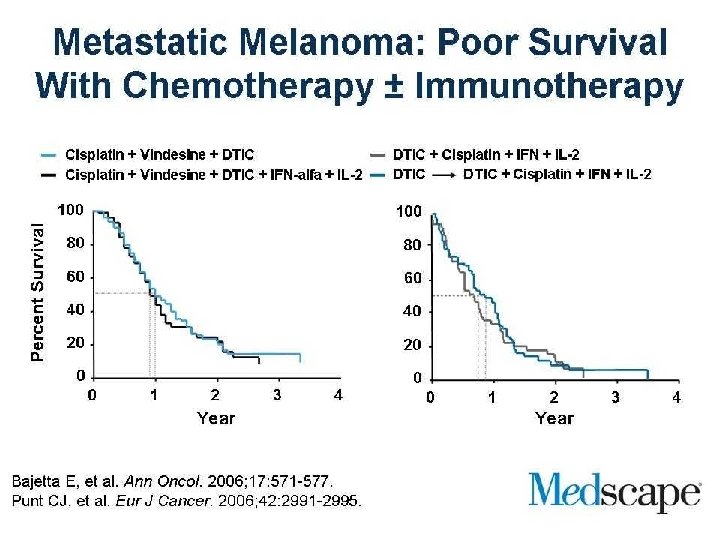
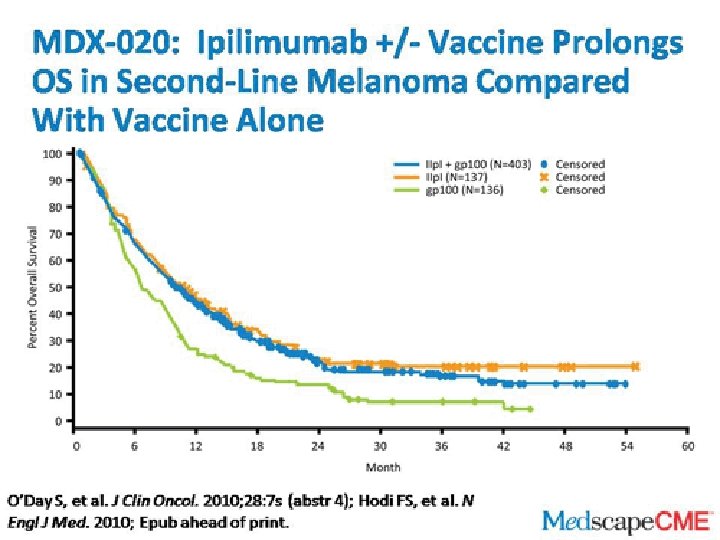
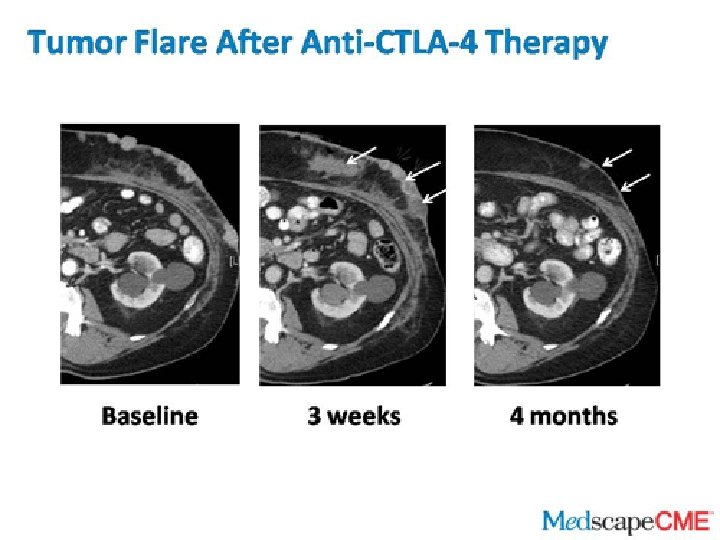
Metastatic Melanoma
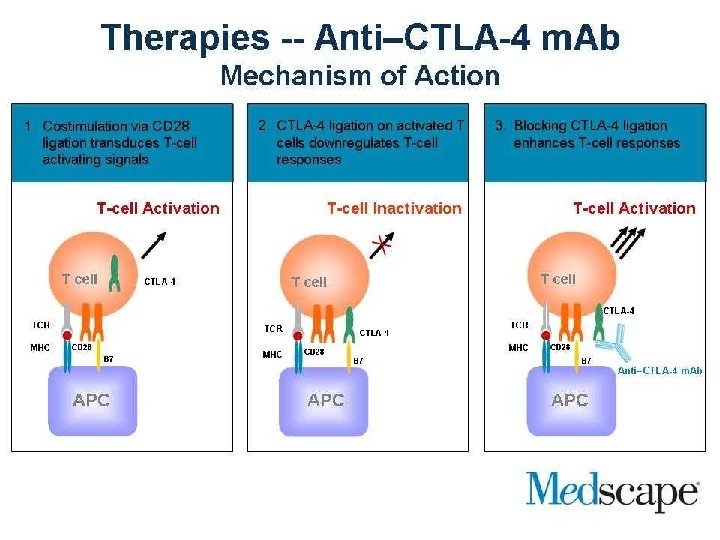

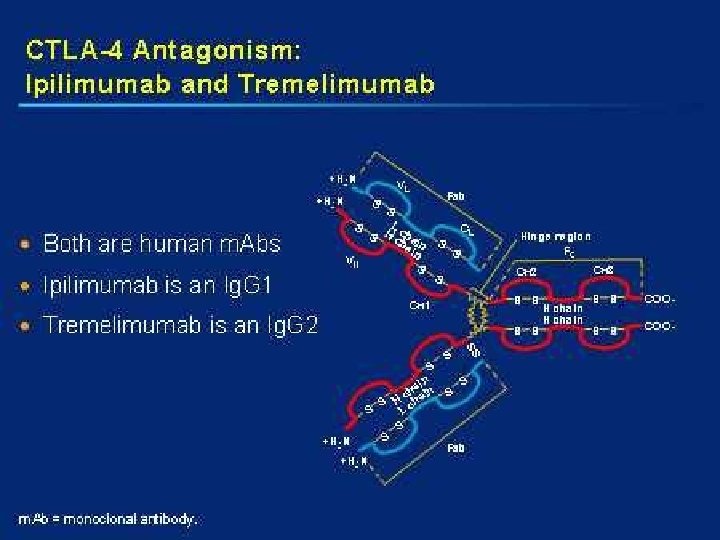
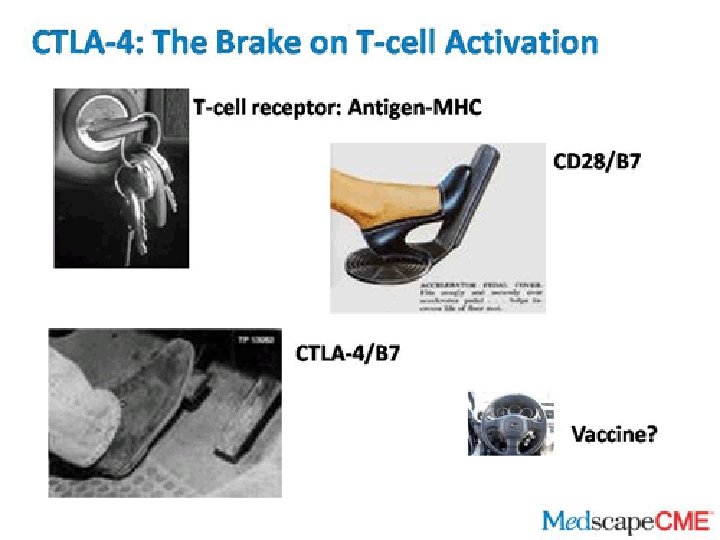
Blocking Antibodies to CTLA 4 MHC Antigen TCR Dendritic cell T cell B 7 CD 28 CTLA 4 Leach DR, et al. Science 1996; 271: 1734 -1736.

Vaccine

Phase I GVAX: Melanoma Vax DTH Met Vasculopathy Pre Met CD 4 CD 8

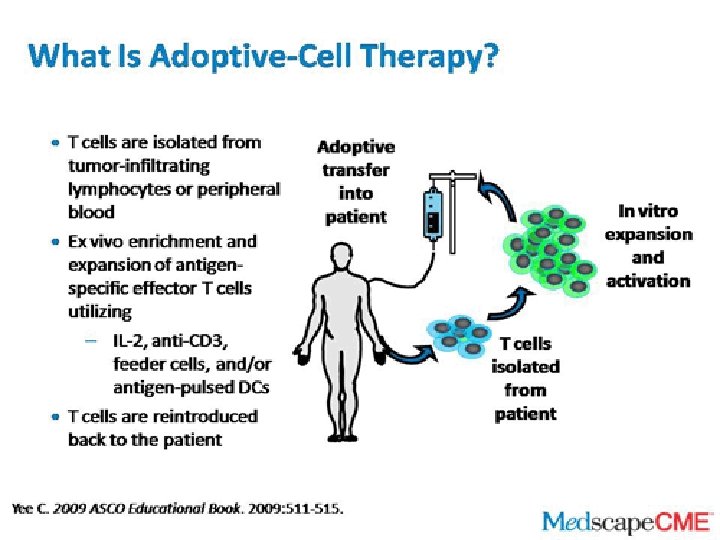
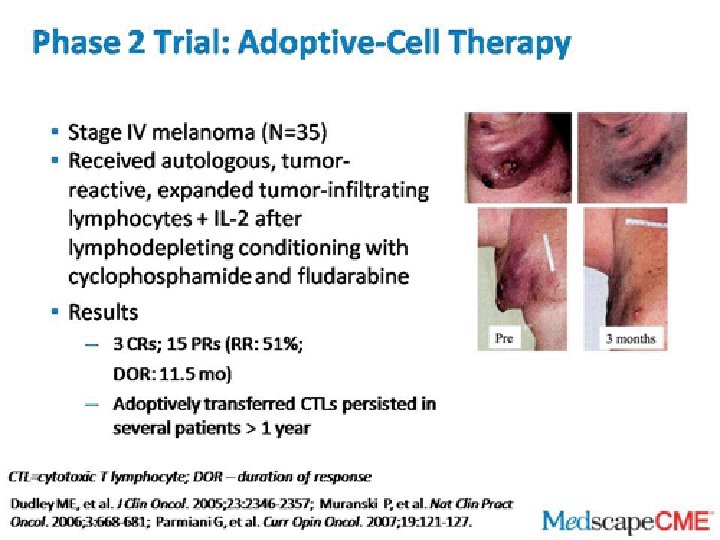
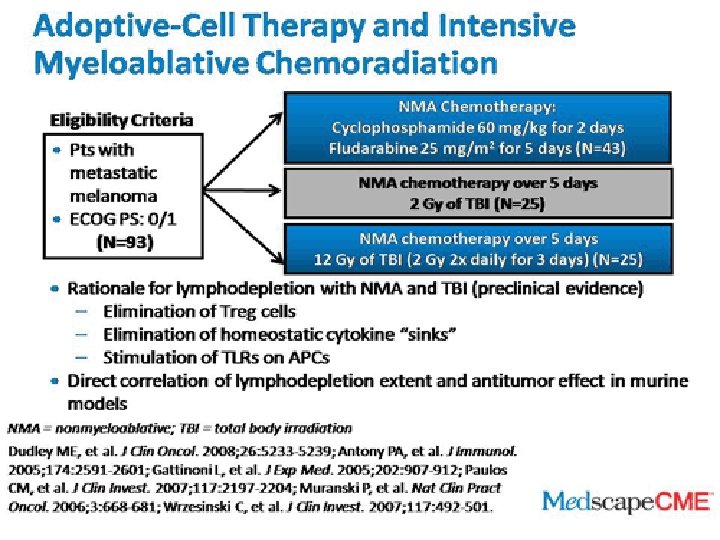
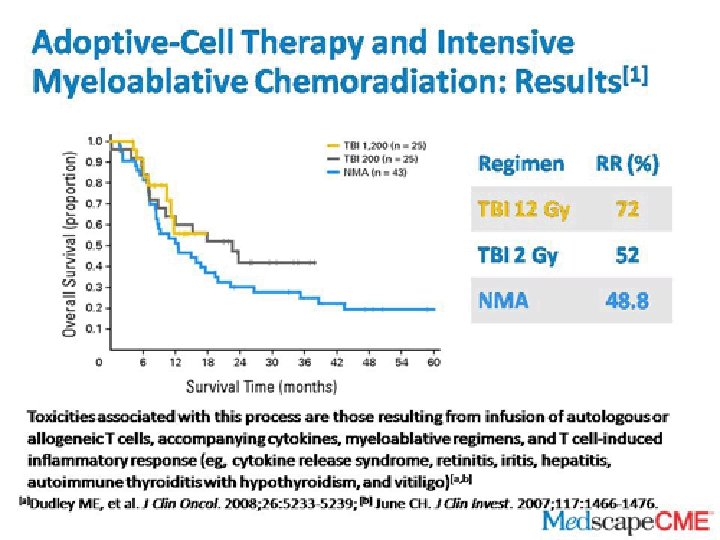
Adaptive Immune Therapy
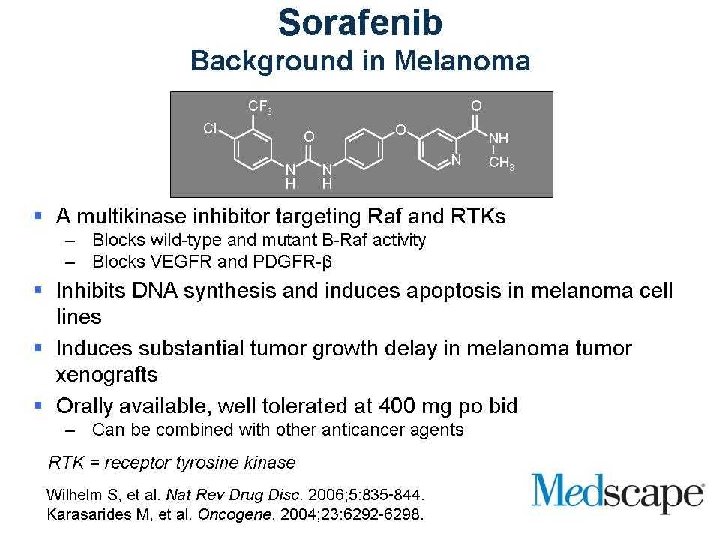
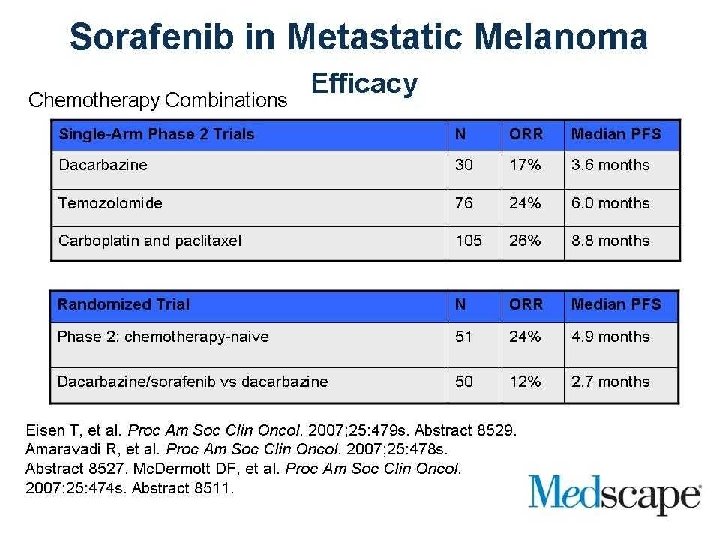
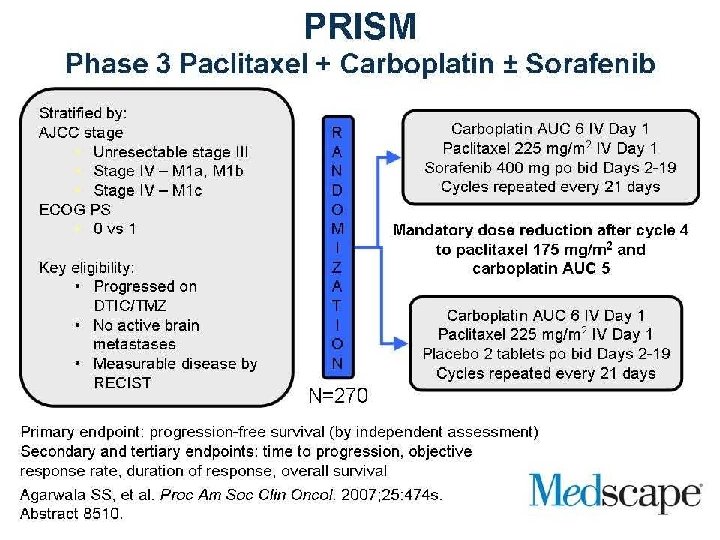

BRAF Inhibitor
- Slides: 92