Pediatric Leukemias Resident Education Lecture Series Cancer of





; no longer")






 Intermediate-high")


















![Promyelocytic Leukemia: M 3 n n Characterized by a translocation [t(15; 17)] that fuses](https://slidetodoc.com/presentation_image_h/7f555e5cd840737c36b77f1c910311ea/image-33.jpg "Promyelocytic Leukemia: M 3 n n Characterized by a translocation [t(15; 17)] that fuses")









- Slides: 42
Pediatric Leukemias Resident Education Lecture Series
Cancer of the bone marrow Major types n n n Leukemia incidence: 4. 1 cases/100, 000 children < 15 years ALL most common; 2000 cases/year (we see 30 -40 cases/year) AML @ 500 cases/year (we see ~6) CML < 100 cases/year, and CLL not seen JMML even less common Factoids n n Typically presents with s/s of anemia, fever, bone pain, bleeding/bruising, HSM/LAD (less in AML; large spleen in CML) Probable genetic component based on twin studies; n linked to trisomy 21, Fanconi, p 53 mutations, Bloom, AT, ionizing radiation, and benzene
Definitions n Marrow n n n M 1: < 5% blasts in normocellular marrow (remission marrow) M 2: 5 -25% blasts M 3: > 25% blasts (definition of leukemia) n CNS* (varies by protocol & disease) n n CNS 1: cytospin (-), independent of cell count CNS 2: cytospin (+), <5 WBC on count CNS 3: cytospin (+), >5 WBC; or CNS sxs Traumatic: this is worse than CNS 2!
ALL: TREATMENT ERAS n n n 1945 -55 1955 -65 1965 -75 1975 -85 1985 -95 1995 -2005 % cured single agents < 1 combination therapy 5 CNS “prophylaxis” 45 tumor biology 50 intensification therapy 75 molecular biology 80 pharmacology genome polymorphisms
Estimated Survival Percentage Improved Survival in Childhood ALL by Study Era Years From Study Entry
ALL subtypes n n Formerly L 1, L 2, L 3 (morphology); no longer used (L 3 morphology = mature B, aka Burkitt) Now surface markers n B-lineage: n n n 85% Early pre-B 57%; pre-B 25% T-ALL: 13% B (mature): 1 -2% (surface Ig) True biphenotypic is bad; a few T or AML marks in o/w classic ALL is fine And molecular subsets
ALL: EARLY CHEMOTHERAPY n Variable ability of drugs to induce remission: n n n n Prednisone Vincristine Asparaginase Methotrexate Mercatopurine Cyclophosphamide 60 % 20 % Drugs good for inducing remission were less effective for sustaining remission
Early Combination Chemotherapy n Induction n n Post-induction n n Prednisone + vincristine PV + asparaginase PVA + daunorubicin Methotrexate + mercaptopurine MM + prednisone + vincristine 84 % 94 -98 % 98 -99 % 5 mos 12 -18 mos 95 % of patients still relapsed, frequently only in the csf
CHEMOTHERAPY for ALL n n n 1967 ASPARAGINASE CYCLOPHOSPHAMIDE MERCAPTOPURINE METHOTREXATE PREDNISONE VINCRISTINE n n n 2004 ASPARAGINASE CYCLOPHOSPHAMIDE CYTOSINE ARABINOSIDE DEXAMETHASONE DOXORUBICIN ETOPOSIDE METHOTREXATE MERCAPTOPURINE PREDNISONE THIOGUANINE VINCRISTINE
CNS “PROPHYLAXIS” STUDY n ST J # PTS # CNSRL # CCR I-III 41 15 7 V: + CSXRT 35 3 18 6: + CXRT/it MTX 45 2 23 - CXRT 49 33 7 C = cranial; CS = craniospinal; XRT = radiation; it = intrathecal CNSRL = CNS relapse; CCR = continuous complete remission Subsequent studies have shown similar results with intrathecal treatment alone. XRT now reserved for patients with CNS leukemia and patients with higher risk T-ALL.
Intensive Chemotherapy n Postulate: early intensive chemotherapy with a combination of drugs will improve cure by n n n more rapid elimination of sensitive cells prevention of the development of resistance treatment of resistant cells
TREATMENT STRATEGIES FOR ALL STANDARD I CNS MODERN I INTENSIVE CNS
SUCCESSFUL INTENSIFICATION FOR ALL: WHAT’S INSIDE THE BOX? n n Weekly asparaginase (DFCC) Intermediate-high dose methotrexate (MCCC; POG/CCG) Delayed reinduction-intensification (BFM/CCG) Multiple rotating pairs of drugs (MCCC; POG) All of these improved cure rates to 70 -80%
Favorable Prognostic Factors in ALL n n n AGE 1 -9 WBC lower Gender female Chromosomes t(12; 21), hyperdiploid Treatment response rapid Residual disease (MRD) less
Genetic Heterogeneity in Childhood ALL: St. Jude Children’s Hospital
B-Precursor ALL: Genotype and Outcome: Children’s Oncology Group 100 Probability Trisomies 4, 10, 17 (n = 746) TEL (n =176) 80 t(1; 19) (n = 139) 60 t(4; 11) (n = 44) 40 4 Yr EFS (%) Tris 4, 10, 17 92. 1 TEL 89. 0 t(1; 19) 68. 9 t(4; 11) 49. 9 t(9; 22) 27. 5 20 0 0 1 2 3 4 t(9; 22) (n=132) SE (%) 1. 1 3. 1 4. 1 11. 2 4. 4 5 6 7 8 9 10 Years Followed 11 12 13 14 15 16 10/2001
Residual Disease Monitoring at End Induction: Flow Cytometry Dx POG ALin. C 17 to Date: 1016 samples received 95% compliance MRD Sensitivity 1/1000 - 1/10, 000 24 hr turn around d 29 Tumor 28. 6% positive median. 069%
PROGNOSTIC VALUE OF MRD IN CHILDHOOD ALL % RFS MONTHS van DONGEN L 352: 1731, 1998
MINIMAL RESIDUAL DISEASE and RELAPSE RISK END INDUCTION MRD- WEEK 14 WEEK 32 RR 7% RR 2/8 n=123 RR 10% 14 MRD + n=42 RR 43% 8 18 4 RR 68% RR 4/4 COUSTAN-SMITH BLOOD 96: 2691, 2000
GENETIC CONTEXT OF MRD MAY BE IMPORTANT MRD+ End Induction Overall 1972 13. 0% 21. 8%
COG ALL Risk Groups 2004: B-Precursor ALL • • • NCI Risk Groups Trisomies 4, 10, & 17 TEL/AML 1 CNS Disease MLL Slow Early Response End of Induction MRD BCR-ABL Chromosomes <45 Induction Failure Low Risk Standard Risk High Risk Very High Risk
Principles of Cure n n n Cure depends upon a complex interaction of patient, disease and treatment-related factors Treatment of all patients with similar regimens risks both overtreatment and undertreatment of individuals Understanding differences in tumor and host genetics (polymorphisms) will be crucial to individualization of therapy
Still an evil disease AML
AML subtypes M 6 M 1 M 4 and M 4 eo M 3 M 7
ACUTE MYELOCYTIC LEUKEMIA: AML M 0 M 1 M 2 M 3 M 4 M 5 M 6 M 7 undifferentiated AML without differentiation AML with differentiation promyelocytic leukemia myelomonocytic leukemia erythroleukemia megakaryocytic leukemia
Prognostic factors n n n n Bad Good n WBC > 100, 000 M 4 eo (inv 16) n Secondary M 6 n Monosomy 7 (7 q-) M# = t(15; 17) n ? Very young Matched sibling transplant up-front n ? Splenomegaly n ? M 4 and M 5 Down Syndrome n ? M 1 w/o Auer rods ? t(8; 21) (latest paper says no) ? Rapid CR Ugly EFS ranges 45 -80%
AML: INDUCTION THERAPY n n Two cycles of cytosine arabinoside + daunorubicin +/-thioguanine and other agents gives remissions in 70 -90% Timed sequential therapy (giving the second cycle at a specified time) does not the increase remission rate but does increase long-term cures when compared to waiting for marrow recovery (or failure) before giving the second cycle (Blood 87: 4979, 1996)
AML: Post-induction Therapy n n Chemotherapy alone has given 30 -50 % cure rates. Cure is higher after timed-sequential induction therapy (42% vs. 27%). Short (4 -12 months) of post-induction therapy is adequate CNS leukemia is less common than in ALL; ‘prophylaxis’ may be accomplished with high dose Ara-C +/- intrathecal Ara-C
AML: Bone Marrow Transplantation n Bone marrow transplantation from a matched sibling donor during first remission gives better cure rates than chemotherapy (50 -60 % vs. 30 -50 %) Autologous BMT during first remission gives results similar to chemotherapy BMT from a matched sibling in second remission gives 30 -40 % cure rate but is limited by the difficulty in achieving second remission.
AML Treatment Issues n n 50% incidence of serious bacterial infection: therefore use of G-CSF accepted New protocol is European-based and returns to the old high-dose Ara-C, with the addition of myelotarg (anti-CD 33, aka gemtuzumab)
Special circumstances n n Granulocytic sarcoma Down syndrome n n n Increased incidence of all leukemias; ALL still > AML total, but RELATIVE increase of AML Do not use intensive timing (increased toxicity with therapy), but OK to use anthracyclines even with CHD M 7 AML most often Transient Myeloproliferative Disease occurs in newborn period M 3 (the 15; 17 translocation)
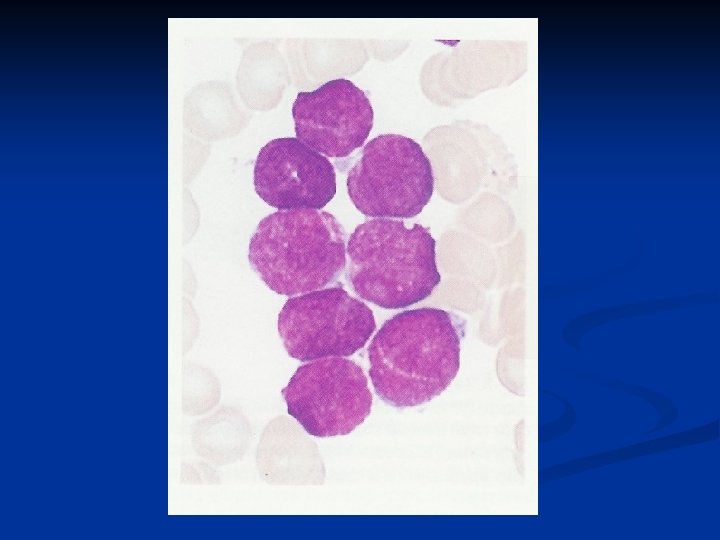
Promyelocytic Leukemia: M 3 n n Characterized by a translocation [t(15; 17)] that fuses the retinoic acid receptor and PML genes The t(15; 17) transcript blocks differentiation that depends upon the normal receptor High dose all-trans retinoic acid overcomes this blockade Arsenic trioxide may cause apoptosis or may induce differentiation in PML cells
Promyelocytic Leukemia: M 3 n n n Induction: all-trans retinoic acid +/- an anthracycline Intensification: anthracycline +/- Ara-C Continuation: intermittent all-trans retinoic acid +/- chemotherapy RESULTS: 90 -95 % remission : 70 -85 % event-free survival : high salvage rate of relapses with retinoic acid, arsenic or BMT Blood 105: 3019, 2005 JClin. Oncol 22: 1404, 2004
CML On which we are going to spend very little time
CML overview n n BCR-ABL fusion protein is generally P 210, whereas Ph+ALL is usually P 190. 3 phases n Chronic n n Accelerated n n Some systemic sxs; peripheral and marrow blasts < 10% (NCI says 5%), thrombo- and leukocytosis Progressive sxs including splenomegaly; blasts 10 (5? ) -30%, baso’s+eo’s > 20% Blast n Extramedullary disease symptoms; blasts > 30%, blasts that look like ALL or AML
CML treatment n Gleevac: aka STI 571, aka imatinib mesylate tyrosine kinase inhibitor that blocks the function of the BCR-ABL fusion protein n n Additional chemo required if disease has progressed n n Morphologic vs cytogenetic vs molecular remission IFN, Ara-C, hydroxyurea Transplant still the Rx of choice for Peds
JMML n n n n Juvenile myelomonocytic leukemia Sometimes called JCML Think of it as stem cell leukemia, but it acts like an MDS more than a leukemia Associated with NF 1 (10+%) Young kids (nearly all < 4; most < 2) Lab findings include high Hgb. F, hypersensitivity to GM-CSF (in vitro), monosomy 7, NO BCR-ABL, < 20% blasts + pro’s (marrow or peripheral), and monocytosis (can have a very high total WBC) Usually treated with SCT, although very often fatal
From ABP Certifying Exam Content Outline n n Pancytopenia 1. General aspects Recognize that a bone marrow aspirate is necessary in the evaluation of a child with multiple pancytopenias
From ABP Certifying Exam Content Outline, continued n n n n WBC disorders b. Acquired (leukemia) Understand that aplastic anemia and childhood leukemia may both present with purpura, pallor, and fever Know that the absence of blasts in the peripheral blood of a patient with pancytopenia does not rule out the diagnosis of leukemia Recognize bone pain as a symptom of leukemia Understand that most patients with acute lymphoblastic leukemia will be cured of their disease using current treatment strategies Identify the central nervous system and testicles as important sites of relapse of acute lymphoblastic leukemia Identify Down syndrome as a disease with an increased risk of leukemia
Credits n Meghen Browning MD Bruce Camitta MD Anne Warwick MD MPH