Brain Tumors in Pediatrics Resident Education Lecture Series

Brain Tumors in Pediatrics Resident Education Lecture Series

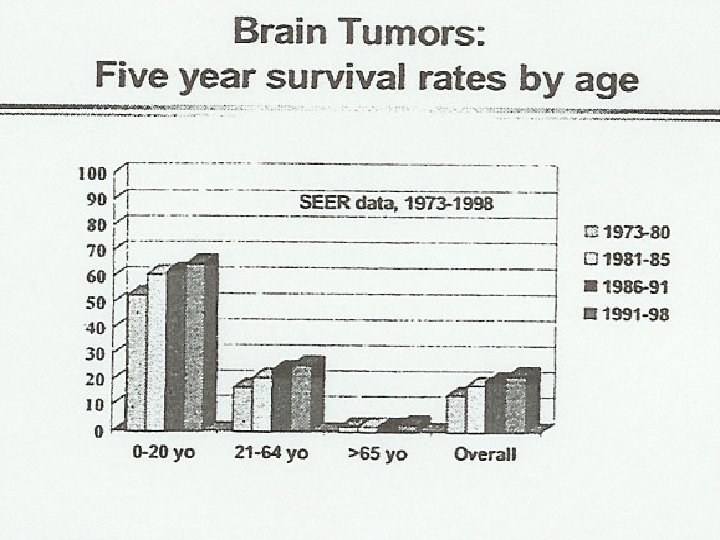
Brain Tumors - Background ¬ ¬ ¬ 20 -30% of cancers in children 2500 -3000 new diagnoses/year 2 nd most common neoplasm Most occur before age 10 years Male/Female = 1. 3/1. 0 60 -70% 5 year survival

Relative Incidence of Brain Tumors in Children Table 25 -1. Approximate incidence of common CNS tumors in children. Pizzo & Poplack
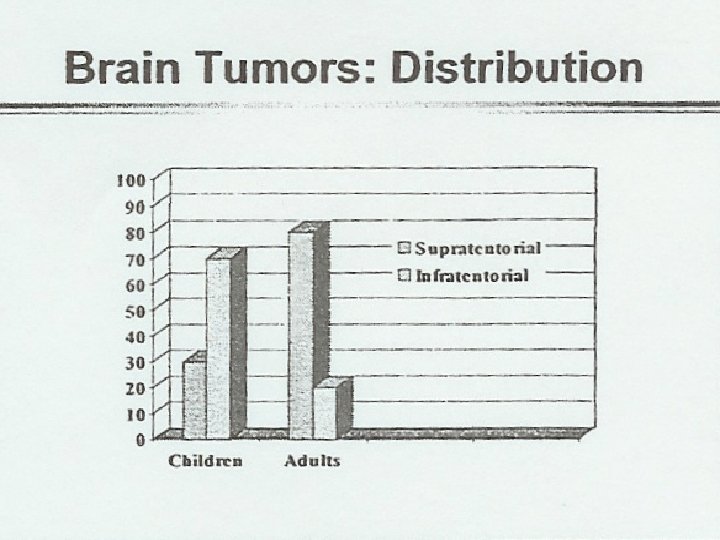

Location – Supra vs. Infra ¬ Supratentorial Ø Ø Ø Astrocytoma, low grade Astrocytoma, high grade Ependymoma Mixed glioma Ganglioma Oligodendroglioma PNET Choroid plexus tumor Meningioma Germ Cell Tumors Other 25 -40% 8 -20% 6 -12% 2 -5% 1 -5% 1 -2% 1 -2% 1 -3%
")
Location – Supra vs. Infra ¬ Infratentorial Ø Ø Ø 45 -60% Medulloblastoma (PNET) 20 -25% Astrocytoma, low grade 12 -18% Ependymoma 4 -8% Brain stem glioma, high grade 3 -9% Brain stem glioma, low grade 3 -6% Other 2 -5%

Brain Tumors - Signs/Symptoms ¬ Increased intracranial pressure - symptoms Ø Ø Ø Ø Ø Headache (am) Nausea/vomiting (am) Double vision Head tilt Decreased alertness Lethargy/irritability Poor feeding, FTT Endocrine dysfunction Unexplained behavior changes - affect, motivation, energy level

Brain Tumors – Signs/Symptoms ¬ Increased ICP – Signs Ø Ø Ø Papilledema, optic atrophy Loss of vision OFC (head circumference) increased Bulging fontanelles, spreading sutures “Setting sun” sign (Parinaud syndrome) Increased blood pressure, low pulse herniation?

Posterior Fossa & Brainstem Tumors - Clinical Features Posterior Fossa primary ¬ Ataxia ¬ Tremors ¬ Dysarthria ¬ Stiff neck ¬ Papilledema Brainstem primary ¬ Extremity weakness ¬ Cranial nerve signs – double vision – facial weakness – swallowing dysfunction

Hemispheric Tumors – Clinical Features ¬ ¬ Hemiparesis Hemianopsia Aphasia Seizures

Treatment Tumor Type Surgery Medulloblastoma +++ Low grade astro +++ cerebellar +++ optic glioma NO High grade astro/GBM +++ Brain stem glioma (exophytic) Ependymoma +++ Germ cell tumor ? bx XRT Cr. Sp focal ? ? ? ? +++ focal +++ Chemo +++ ------? ? ? ---+++

Treatment - Surgery ¬ In general, needed for diagnosis - exceptions: GCT, BSG ¬ Ideal is gross total resection Balance prognosis vs. morbidity ¬ Debulking, shunts, reservoirs - for symptom/ICP reduction, therapy

Treatment – Radiation Therapy ¬ Potential for use in all brain tumors – exceptions: choroid plexus tumors ¬ Neuro-axis prophylaxis (cranio-spinal rx) – if tumor disseminates via CSF ¬ Concerns for long term effects – – – neuro-cognitive hearing secondary cancers endocrine skeletal growth

Therapy - Chemotherapy ¬ Adjunct therapy in most cases – particularly in GCT, medulloblastoma ¬ Of interest in young children – (avoid or prolong XRT) ¬ Blood brain barrier may be limiting – Newer studies suggest this may not be so – Local delivery via pumps/reservoir/IT

Medulloblastoma/PNET Similar histology, different tumor names based on location. – Therapies vary ¬ Medulloblastoma ¬ PNET ¬ Pineoblastoma - posterior fossa - supratentorial - pineal region ¬ median age 5 years ¬ M: F = 2: 1 ¬ propensity to disseminate – 1/3 with metastatic disease at diagnosis

Medulloblastoma Prognostic Factors ¬ ¬ ¬ Age - Younger tend to do worse Extent of resection Non-posterior fossa tumors Non-localized disease Standard risk 70 -80% 5 yr survival High risk 50% what are risk groups?

Medulloblastoma ¬CSF dissemination – check for leptomeningeal spread – brain/spine MRI, LP ¬ Can spread to lung, liver, BM, bone, LN’s – rare ¬ Difference between supratentorial PNET (s. PNET), medulloblastoma, and pineoblostoma?

Ependymoma ¬ 10% of childhood brain tumors ¬ Median age = 3 -4 yrs ¬ 2/3 of primary in posterior fossa ¬ May have leptomeningeal spread of brain/spine, CSF ¬ Prognostic factors: – Extent of resection!!! – Age: some reports of better survival if > 5 -7 years at diagnosis – Histology - MRI

Ependymoma - continued ¬Extent of resection most important – Near to gross total resection 50 -75% – Less than NTR 0 -30% ¬Radiation therapy helps survival – Reduces local recurrence ¬Chemotherapy has not shown efficacy ¬Recurrence is rarely fixable

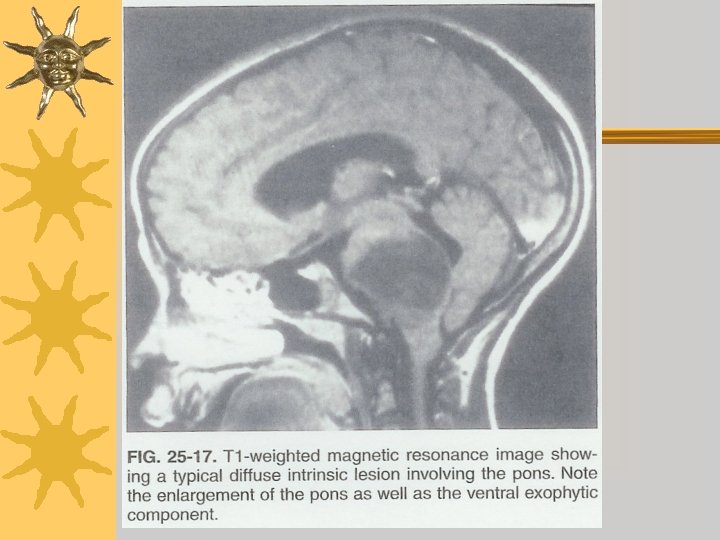
Brain Stem Gliomas ¬Diffuse intrinsic pontine gliomas – median survival = 6 -9 months – death within 2 years > 90% – Radiation - transient clinical improvement ¬Low grade gliomas – tectal, exophytic, extra-medullary – highly enhancing on MRI – more indolent

Low Grade Astrocytoma/Glioma ¬ 30 -35% of CNS tumors – 40 -50% supratentorial, virtually anywhere ¬ M: F = 2: 1 ¬ Association with NF-1 – more indolent course ¬ GTR >90% 5 year survival ¬ RX – Radiation – Chemo if symptomatic, progressive, or recurrent

Brain Tumors in < 3 year olds ¬ 60 -70% supratentorial ¬ XRT has significant neuro-cognitive effects ¬ Goal of therapies: – Delay XRT to at least 3 yrs old with chemotherapy most relapse prior to XRT ¬ Current study – – Short course (16 wks) chemo 2 nd look surgery Focal (conformal) XRT Maintenance chemotherapy

Complications From Tumor/Therapy ¬Neurological deficits – limb paresis • Rehab/PT/OT, support – swallowing/speech dysfunction • ENT, Speech therapy • Nutrition issues – neuro-cognitive deficits • School/education issues • Social interaction issues – endocrine dysfunction – end-organ damage • kidney, liver, hearing, neuropathy


From ABP Certifying Exam Content Outline ¬ Recognize the signs and symptoms of craniopharyngioma ¬ Recognize the clinical manifestations of brain tumor ¬ Recognize the physical characteristics of a headache due to increased intracranial pressure ¬ Differentiate the clinical manifestations of spinal cord compression (eg, from a tumor) from those of other myelopathies, and evaluate appropriately

Credits ¬Sachin Jogal MD
- Slides: 28