PDLS The Pediatric Patient Unique Anatomic and Physiologic



 Cardiopulmonary Failure")

















 fracture -")

- Slides: 30
© PDLS : The Pediatric Patient Unique Anatomic and Physiologic Features
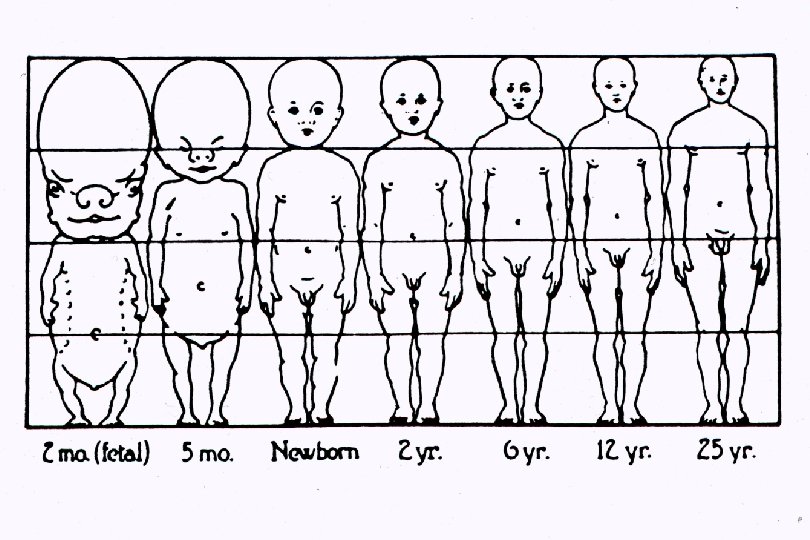
Body Size and Composition height and weight increase throughout childhood less protective fat and muscle large surface area predisposes to hypothermia
Body Proportions body proportions account for unique injury patterns in childhood large head increases risk of head injury accompanying any other major traumatic injury large, “unprotected” intraabdominal organs increases risk of liver, spleen, bowel injury following less severe trauma
Etiologies of Cardiopulmonary Failure Many Etiologies Respiratory Failure Circulation Failure (shock) Cardiopulmonary Failure
Respiratory Distress and Failure respiratory distress: increased work of breathing respiratory failure: inadequate oxygenation and/or ventilation to meet metabolic needs
Signs of Respiratory Distress and Failure signs of respiratory distress: - tachypnea, tachycardia - retractions (intercostal, superclavicular, nasal flaring) - grunting signs of respiratory failure - altered mental status - poor color - hypotonia
Infant with Increased Respiratory Effort Note use of intercostal and accessory muscles
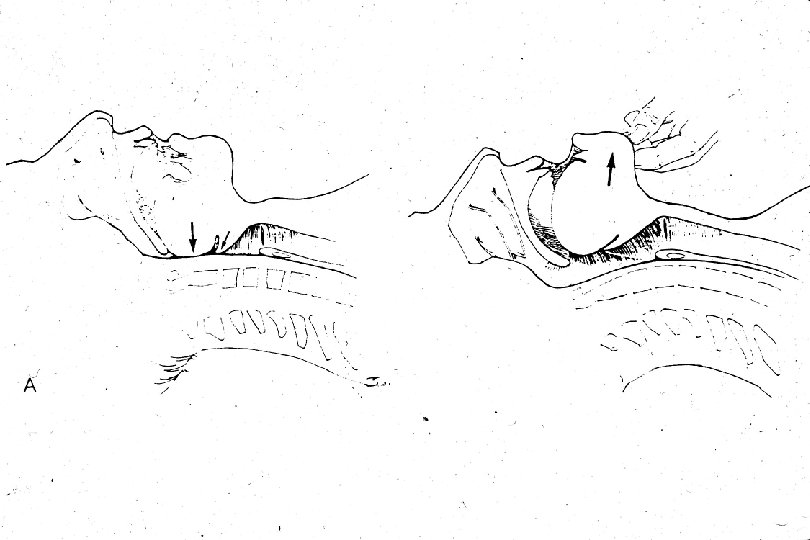
Features of the Pediatric Upper Airway large occiput small mouth large tongue anterior and cephalad larynx angled cords large, floppy epiglottis overriding airway narrow cricoid ring
Neonatal Airway Large head Small nares Large tongue High glottis Overhanging epiglottis Angled cords Narrow cricoid region
Airway Equipment for the Young Pediatric Patient straight blade: compresses large tongue and mandibular tissue uncuffed tube in children < 8 years tube size = age years +4 4 (for children over 2 years)
Features of the Pediatric Lower Airway short trachea narrow caliber of all airway structures compliant chest wall horizontal ribs diaphragm as a respiratory muscle
Features of the Pediatric Cardiovascular System shock: defined as the clinical state of inadequate perfusion to meet metabolic needs degree of shock is based on evaluation of the end organs of perfusion: - skin (color, temperature, cap refill) - CNS (developmentally appropriate behavior, lethargy, anxiety) - central vs peripheral pulses - renal (urine output)
Simultaneous Palpation of Proximal and Distal Pulses
Features of the Pediatric Cardiovascular System cardiac output is rate dependent: infants cannot increase stroke volume to compensate for shock smaller total blood volume: 80 -100 cc/kg increased parasympathetic output: increased vagal tone
Hemodynamic Changes with Blood Loss
Pediatric Vital Signs mean heart rate decreases with age tachycardia is an early and nonspecific sign of shock mean blood pressure increases with age blood pressure is usually normal even in a child with moderate-severe hypoperfusion increased peripheral vascular tone allows for normal blood pressure until end-stage shock vital signs not helpful in gauging degree of shock in children
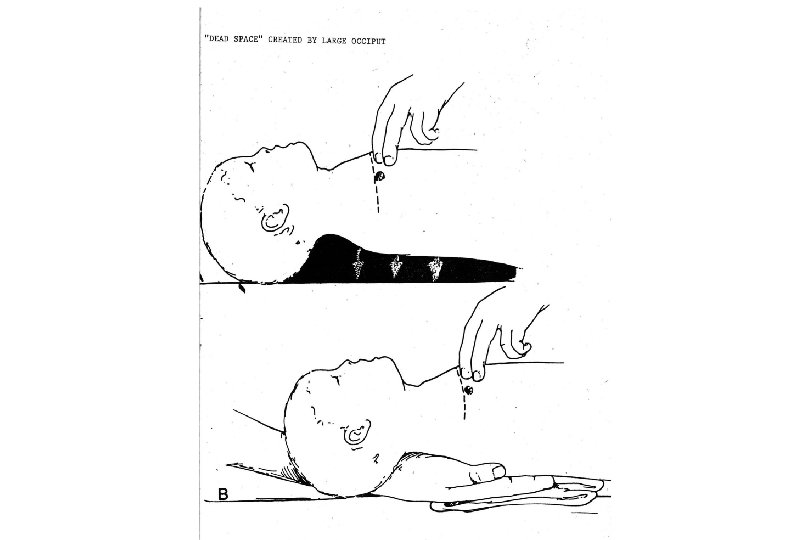
Pediatric Cervical Spine fulcrum is at C 2 -3 growth plate of dens weak neck muscles large head increases momentum SCIWORA because of ligamentous laxity most fractures occur at C 1 -2 difficulty with immobilization: large head/small chest allow for excessive flexion in supine position
Head Injury in the Young Pediatric Patient skull is more compliant offers less protection to the brain open sutures and fontanel mobile middle meningeal artery intracranial bleeds occur without accompanying fracture intracranial bleed can cause shock
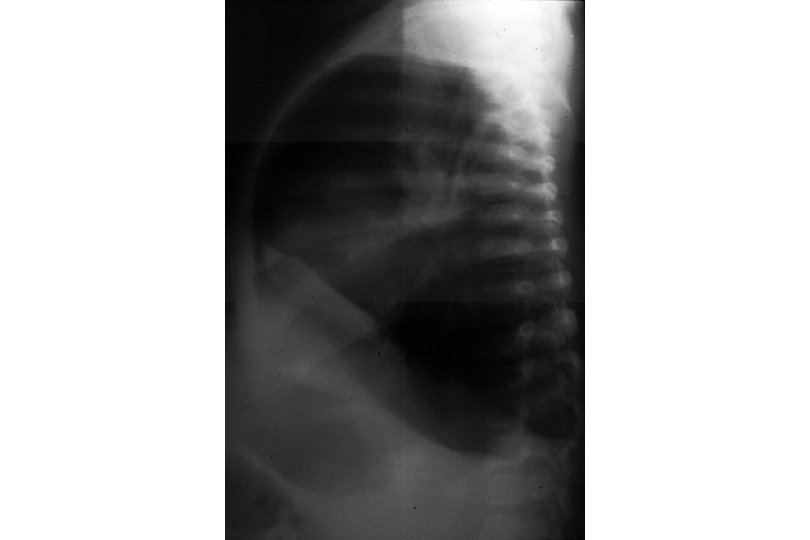
Features of the Pediatric Abdomen thinner abdominal wall with less fat and muscle decreased anterior-posterior diameter large liver and spleen extend below ribs kidney contains less perinephric fat gastric distention (with ventilation or crying) can present as a tense abdomen
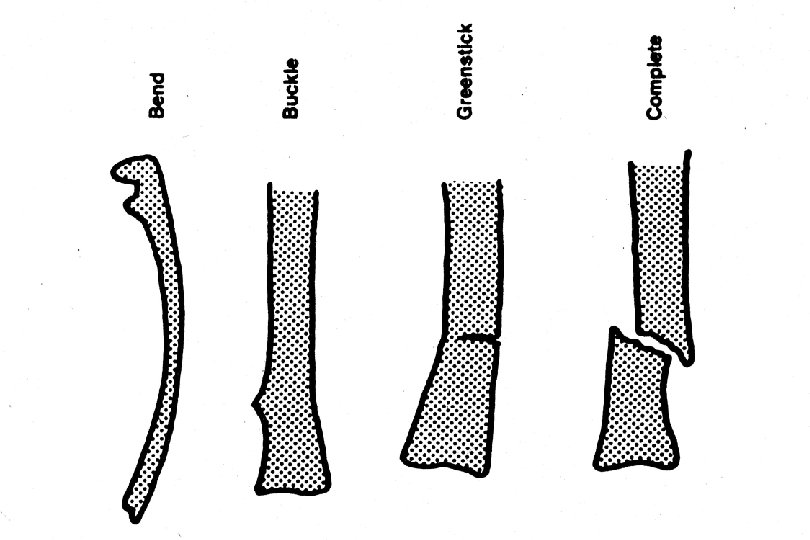
Skeletal System Fractures seen exclusively in children: - growth plate (Salter Harris) fracture - torus fractures - bowing fractures - greenstick fracture
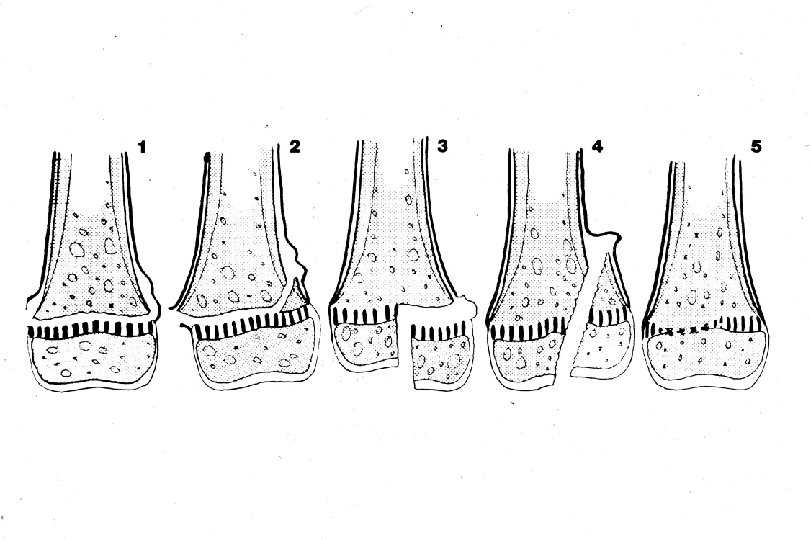
Skeletal System physis is site of growth physis is the weakest part of bone physis is composed of cartilage and separates epiphysis from metaphysis fractures of the physis are described by the Salter Harris Classification