Past history No underlying disease No drugs or

 1 x 3 (>2 months) • Pyridostigminine(60)")

































 •")

















 S : ตนด ไมม n/v ไมมหอบเหนอย ปวดแผล O: BT 37. 2")
 S : ตนด ไมม n/v ไมมหอบเหนอย ปวดแผลลดลง กนได O: BT 36.")


- Slides: 62
Past history • No underlying disease • No drugs or food allergy • No smoking and alcohol drinking • No Hx of surgery or previous anesthesia • FC I
Past history • Current medication • Prednisolone(5) 1 x 3 (>2 months) • Pyridostigminine(60) 1 tab PO q 6 hrs (240 mg/day)
Physical examination Vital signs BP 100/62 mm. Hg PR 71 BPM BT 37°C RR 16 breaths /min • BW 44 kg, Height 155 cm (BMI 18. 4 kg/m 2) • GA : A Thai female, good consciousness, well co-operated, not pale, no jaundice
Physical examination • HEENT : No ptosis, not pale, no jaundice, no buffalo hump, no hoarsness , no thyroid gland enlargement • Pulmonary : no dyspnea , no tachypnea , no use of accessory muscle , clear and equal breath sound both lungs • CVS : Pulse full & regular , no heaving, no thrill, normal S 1&S 2, no murmurs
Physical examination • Airway examination : Limit neck of motion : No Thyromental distance > 6 cm Mouth opening > 3 cm Prominent incisor : No Mallampati grade : grade 1
Physical examination • Abdomen : soft, not tender, liver & spleen can not palpable, no abdominal striae • Extremities : no deformity, no pitting edema • Neuro : E 4 M 6 V 5, no facial palsy, full EOM, Pupil 2 mm RTLBE, normal gag reflex, motor grade V/V all, DTR 2+all
Myasthenia gravis • Myasthenia gravis is an autoimmune disease characterised by muscular weakness and fatigability.
Diagnostic tests • History and clinical exam • Electrophysiologic test • Pharmacologic test • Serologic test
Differential diagnosis
Yao & Artusio’s Anesthsiology, 7 th Ed , 1153 -1167
Yao & Artusio’s Anesthsiology, 7 th Ed , 1153 -1167
Yao & Artusio’s Anesthsiology, 7 th Ed , 1153 -1167
R 1 Investigations
Investigations • Complete blood count >> Baseline Hct, Platelet • Electrolyte, FBS >> Electrolyte disturbance, Hyperglycemia • BUN/Creatinine >> Renal function • Imaging : Chest X-Ray & CT chest >> Lung lesion, Thymus glands size • Pulmonary function test >> Lung function, FVC
Investigations • CBC: Hb 13 gm/dl, Hct 41. 2%, Platelet 327, 000/mm 3 • Electrolytes: Na 140, K 4. 03, Cl 99. 2, CO 2 27. 8 • BUN: 16. 1 mg/d. L Cr: 0. 61 mg/d. L • FBS : 82 • TFT : TSH 0. 62, FT 3 2. 53, FT 4 1. 18
Investigations • CXR
Investigations • CT-Chest : • Thymus size 1. 2 x 2 cm. Otherwise are unremarkable
Investigations • EKG : NSR, No ST-T abnormalities
R 2 Problem list
Problem list • Female 20 years-old • Myasthenia gravis Class IIa • Secondary adrenal insufficiency
ASA classification ASA class II FC I
R 2 Preoperative evaluation
Preoperative evaluation Myasthenia gravis • Identify Associated diseases • Review of the severity of the patient’s disease and the treatment regimen
Preoperative evaluation Myasthenia gravis • Associated disease >> Autoimmune diseases • Thyroid abnormalities • Rheumatoid arthritis • SLE No associated • Pernicious anemia diseases
Preoperative evaluation Myasthenia gravis • Severity of the patient’s disease • Presentation • Bulbar involvement • Respiratory muscle • The treatment regimen • Medication • Clinical progression after treatment Postoperative ability to protect and maintain a patent airway
Preoperative evaluation Myasthenia gravis • Medical therapies for MG can be classified into three groups: • Anticholinesterase drugs : Pyridostigmine >> Mg/day • Immunosuppressive drugs : Corticosteroid >> Dose&duration • Short-term immunotherapies (plasmapheresis and immunoglobulin)
Preoperative evaluation Myasthenia gravis Leventhal, Orkin, and Hirsch scoring system • a total score of ≥ 10 points identified those patients likely to need postoperative pulmonary ventilation for more than three hours
Preoperative evaluation Secondary adrenal insufficiency • HPA suppression can occur after • 5 daily doses of prednisone 20 mg • > 3 weeks of prednisolone 5 -7. 5 mg • Recovery of HPA function occurs gradually and can take up to 9 to 12 months • HPA suppression can occur with topical, regional, and inhaled steroids • 2 g/day topical steroids • 0. 8 mg /day inhaled steroid Barash's Clinical Anesthesia, 7 th Ed 2013 Stoeltings Anesthesia and Co. Existing Disease 6 th Ed
Preoperative evaluation Secondary adrenal insufficiency • Stress dose steroid Perioperative Steroid Management, Anesthesiology 7 2017, Vol. 127
Preparation & premedication • Advice risk of post-op intubation and mechanical ventilation • Breathing exercise & incentive spirometry • Set OR first case of day (ideally)
Preparation & premedication • Pre op anticholinesterase ? ? ? • Avoid drug interaction • Patient weakness before arrival operating room • Anxiolytic, sedative, and opioid • Increase sensitivity to respiratory depression
Preparation & premedication • • • NPO Inform consent 5%DN/2 1000 ml iv drip 80 ml /hr Hydrocortisone 100 mg iv G/M PRC 1 u ATB Warm iv fluid Large bore IV Force air warmer
R 3 Anesthetic consideration
Response to anesthetic drug • Inhaled Anesthetic Agents • More sensitive to neuromuscular depressant • Slightly greater than 1 MAC depresses (EMG) responses • Sevoflurane > concentration-dependent decrease in T 1 & T 4/T 1 • More effect of neuromuscular depressant in Baseline T 4/T 1 < 0. 9 Barash's Clinical Anesthesia, 7 th Ed 2013, 1065 -1068
Response to anesthetic drug • Muscle relaxant Depolarizing Non-depolarizing
Response to anesthetic drug In MG Nondepolarizing relaxant • Increase sensitivity ( ED₅₀&ED₉₅) • Tritrated in 1/10 of the usual dose • Careful monitoring (TOF monitor) • Avoid long-acting drugs • Reverse by anticholinesterase drugs with carefully • Rocuronium & Sugammadex Barash's Clinical Anesthesia, 7 th Ed 2013, 1065 -1068
Response to anesthetic drug In MG Depolarizing relaxant > Succinylcholine • Resistant to SCH • Usual doses can use with adequate for intubation • May not seen fasciculation • Prior use anticholinesterase may delay SCH metabolism Barash's Clinical Anesthesia, 7 th Ed 2013, 1065 -1068
Response to anesthetic drug • Opioids • At therapeutic range not effect neuromuscular transmission • Central respiratory depression • Short acting opioid c titrate dose • IV anesthetics • barbiturates and propofol are safely use for myasthenic patients • Propofol has theoretic advantages of short duration of action without effect on neuromuscular transmission Barash's Clinical Anesthesia, 7 th Ed 2013, 1065 -1068
Intraoperative management
Choice of anesthesia • GA with ETT with control ventilation • Combine with Thoracic epidural
Intraoperative Monitoring • Standard monitoring • EKG, ETCO₂, NIBP, Pulse oximetry • Special monitoring? • Neuromuscular monitoring Nerve stimulator : TOF ratio • • Use of Neuromuscular blockade Induction/Intubation period Surgical period Reversal of neuromuscular block period
Induction & intubation • IV induction vs Inhalation induction • Muscle relaxant • SCH • Non depolarizing neuromuscular blockers • Avoid long acting • Non muscle relaxant technique
Maintenance • Volatile • TIVA • Regional anesthesia : Thoracic epidural • Reduce dose of other anesthetic drugs • Good for postoperative pain control and improve respiration • Epidural opioids may be use short acting and beware of respiratory depressant
- Monitor NIBP, EKG, O₂sat BP at OR 117/65 PR 72 Fentanyl 50 mcg Plan combined with thoracic epidural >>> Fail
Induction • Fentanyl 50 mcg • Sevo 1 % q 1 -2 breaths up to 8% • N₂O : O₂ 7: 3 (70% N₂O ) Intubation • Propofol 100 mg iv • ETT 7. 5 depth 21 cm • BP 100/65 PR 65
Maintenance N₂O: O₂ 0. 5: 0. 5 Desflurane up to 6% Fentanyl 150 mcg ATB : cefazolin 1 gm iv Iv fluid : acetar 600 ml Urine : 90 ml EBL : minimal Operation time : 3 hr 30 min
Awake extubation
Intraoperative management Leventhal, Orkin, and Hirsch scoring system • Total score < 10 points Low risk for postoperative mechanical ventilation
Awake Extubation Subjective • Follow command • Clear Oro/Hypopharynx • Intact Gag reflex • Head lift 5 sec or sustained hand grip • Adequate pain control • Minimal Expiratory anesthetics Objective • Vital capacity ≥ 10 cc/Kg • Tidal volume > 6 cc/kg • Peak voluntary negative Inspiratory pressure > -20 mm. H₂O • T₁/T₄ > 0. 9 or Sustained tetanic contraction • Alveolar-arterial Pa. O₂ gradient < 350 mm. Hg (Fi. O₂ 1) Barash's Clinical Anesthesia, 7 th Ed 2013
Post operative period • Need for postoperative mechanical ventilation • Adequate pain control • Pulmonary toilet
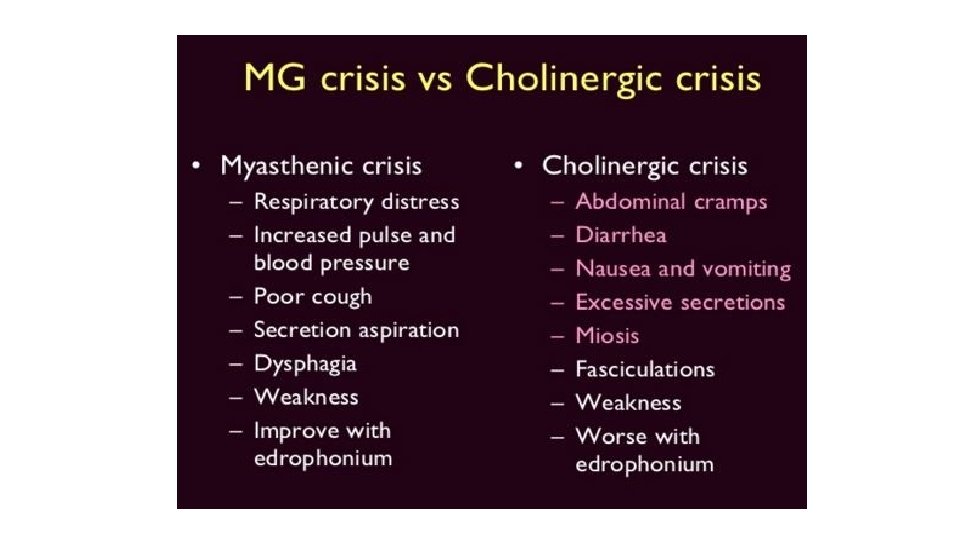
Post operative weakness • Myasthenic crisis • Cholinergic crisis • Residual effects of anesthetic drugs
Cholinergic crisis • Cholinergic crisis results from an excess of cholinesterase inhibitors • flaccid muscle paralysis • Miosis • SLUDGE syndrome (salivation, lacrimation, urinary incontinence, diarrhoea, GI upset and hypermotility, emesis)
Myasthenic crisis • Facial muscles may be slack, and the face may be expressionless • Inability to support the head, which will fall onto the chest while the patient is seated • Gag reflex is often absent, and such patients are at risk for aspiration of oral secretions • bronchospasm with wheezing, bronchorrhea, respiratory failure, diaphoresis, and cyanosis
Post operative(day 1) S : ตนด ไมม n/v ไมมหอบเหนอย ปวดแผล O: BT 37. 2 PR 80 BP 120/ 80 RR 18 pain score 6 -8 A+P: MG: continue Mestinon(60)1*4 Pain control : Mo 4 mg iv prn q 4 hrs, Fentanyl Patch 25 mcg/Hr Tramol(50) 1 tab O prn q 6 hrs. GU : I/O 1372/1390 GI : soft diet Neuromuscular: no muscle weakness Respiratory : clear both lung, breathing exercise Hemato : Hct 40 Vol%
Post operative(day 2) S : ตนด ไมม n/v ไมมหอบเหนอย ปวดแผลลดลง กนได O: BT 36. 8 PR 70 BP 126/ 85 pain score 3 -4 A+P: MG: continue mestinon(60)1*4 Pain control : Fentanyl Patch 25 mcg/Hr Brufen(400) 1 x 3, Para(500) 1 tab O prn q 6 hrs GU : I/O 800/1250 GI : soft diet Neuromuscular: no muscle weakness, no ptosis Respiratory : clear & equal breath sound
Take home message Myasthenia Gravis ØClinical history, pathophysiology, associated diseases ØSeverity classification and treatment regimen ØInteraction with anesthetic drugs ØAnesthetic management and Neuromuscular monitor ØPredicted to post-op need for ventilatory support ØPost operative weakness
THANK YOU