Other Coccidian and Apicomplexan parasites Cyclospora Cyclosporosis v

")









")



, malabsorption and dehydration (Intestinal")




 was previously classified as a protozoa. Currently,")

- Slides: 25
Other Coccidian and Apicomplexan parasites
Cyclospora (Cyclosporosis)
v. The first human cases of Cyclospora cayetanenis were reported in 1979. v It was originally referred to as cyanobacteria -like bodies or coccidianlike bodies (CLB). v The organism was confirmed to be a coccidian parasite with an oocyst structure in 1994.
v. Molecular studies indicate a close relationship to Eimeria, an important veterinary parasite of poultry and other livestock. v. C. cayetanenis has a worldwide distribution, but appears to be especially prevalent in Latin America, the Indian subcontinent, and Southeast Asia. v In developed countries the infections are usually associated with either food borne outbreaks or traveler's diarrhea.
Autoinfection DOES NOT occur
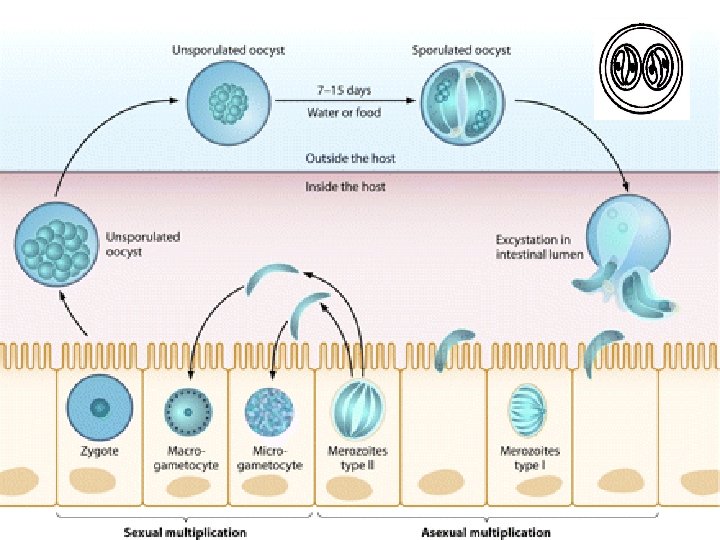
Cyclospora oocyst =2 sporocysts each = 2 sporozoites, 8 -10µ Autoinfection DOES NOT occur Isospora oocyst = 2 sporocysts each = 4 sporozoites. 30 X 12µ Autoinfection MAY occur
Pathogenesis: ØCyclospora primarily infects epithelial cells in the upper portion of the small intestine. ØSymptoms are similar to the gastroenteritis caused by Isospora and Cryptosporidium which typically includes cycles of watery diarrhea and periods of apparent remission. ØAs is also the case for Cryptosporidium and Isospora, the diarrhea caused by Cyclospora in AIDS patients is much more severe than in immunocompetent persons.
Epidemiology: §Soil transmitted infection in endemic areas. §Several outbreaks in the United States and Canada have been associated with food borne transmission [fresh produce imported from endemic areas (South and Central America)]. In particular, berries and leafy vegetables have been identified as the probable contaminated item. §Cases in Europe and Australia have been associated with travel to endemic countries.
Diagnosis, treatment and control: like Isospora.
Diagnosis of Cyclospora & Isospora Stool examination to detect unstained and stained oocysts Unstained oocyst Cyclospora Unsporulated Isospora Stained oocyst by MZN stain Cyclospora Unsporulated Isospora Sporulated Isospora
A B C A: Oocysts of Cyclospora cayetanensis in stained stool smear. B: Oocysts of Cyclospora, unstained stool smear. C: Oocysts from Cryptosporidium in staining stool smear.
Microsporidia (Microspordiosis)
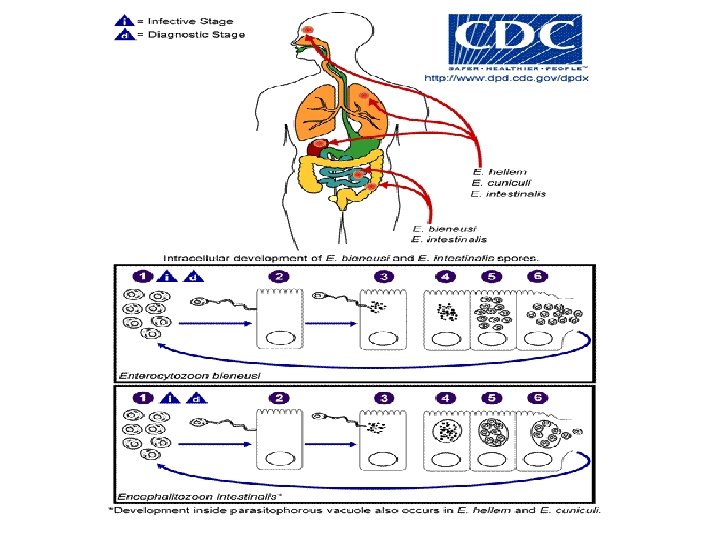
q. The term microsporidia is also used as a general nomenclature for the obligate intracellular parasites belonging to the Kingdom: protozoa, phylum Microsporidia. q. More than 1, 200 species belonging to 143 genera have been described as parasites infecting a wide range of vertebrate (domestic and wild animals) and invertebrate hosts. q. Microsporidia, are characterized by the production of resistant spores that vary in size, depending on the species.
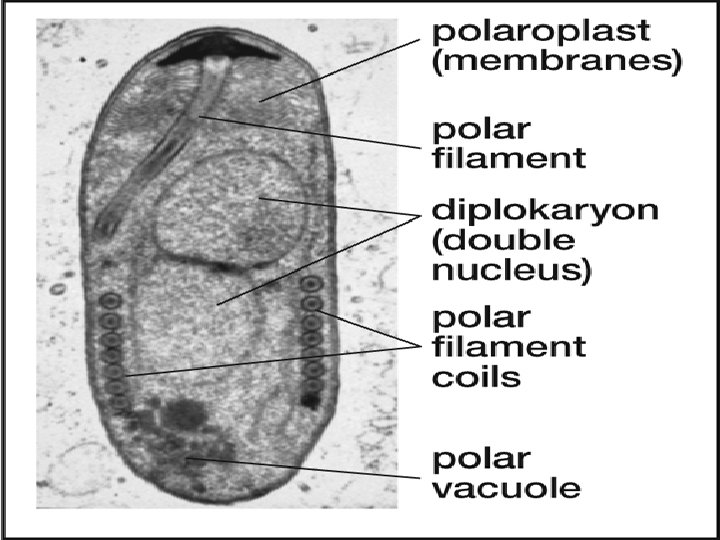
q They possess a unique organelle, the polar tubule or polar filament, which is coiled inside the spore as demonstrated by its ultrastructure. no mitochondria! may be closer to fungi than protozoa! q. There at least 15 microsporidian species that have been identified as human pathogens q. Most Microsporidia develop in the cytoplasm, a few are surrounded by a vacuole.
Pathogenesis: ØHuman microsporidiosis represents an important and rapidly emerging opportunistic disease, occurring mainly, but not exclusively, in severely immunocompromised patients with AIDS. ØAdditionally, cases of microsporidiosis in immunocompromised persons not infected with HIV as well as in immunocompetent persons also have been reported. Ø The clinical manifestations of microsporidiosis are very diverse, varying according to the causal species with diarrhea being the most common.
Clinical manifestations of microsporidiosis Intestinal infection: Most common prolonged diarrhea(AIDS), malabsorption and dehydration (Intestinal microsporidiosis) Ocular infection: Conjunctivitis, keratitis and corneal ulcers(healthy and HIV patients (Ocular microsporidiosis). Generalized muscle weakness: Myalgia , fever , weight loss (Microsporidial myositis). Involves several systems: intestinal , biliary tract, ocular, hepatic , renal and respiratory systems
Mode of infection : uncertain • By ingestion • Ocular exposure, • Inhalation, • Sexual intercourse
Diagnosis: v. Microscopic examination of the stained clinical smears, especially the fecal samples, excreta and body fluids to see the spores microscopically. v. Biopsy v. Transmission electron microscopy (TEM). v. Immunofluorescence assays (IFA). v. Molecular methods (mainly PCR)
Treatment: Microsporidial infections are difficult to treat because of their intracellular habit and the resistant nature of the spores. The treatment of microspordiosis varies according to site of infection and clinical manifestation. Nitazoxanide: intestinal infection Albendazole: intestinal, disseminated infections. Topical fumagillin: ocular lesions
Blastocystis hominis ØIt has been previously considered as yeasts, fungi, or ameboid, flagellated, or sporozoan protozoa. ØRecently based on molecular studies, B. hominis has been placed within an informal group, the stramenopiles. ØStramenopiles are defined; a heterogeneous evolutionary assemblage of unicellular and multicellular protists including brown algae, diatoms, chrysophytes, water molds, slime nets, etc.
Pneumocystis jirovecii previously classified as Pneumocystis carinii) was previously classified as a protozoa. Currently, it is considered a fungus based on nucleic acid and biochemical analysis.
An AIDS patient developed severe watery diarrhoea with no mucus or blood. Stool examination showed no eggs of helminths. Diagnosis was confirmed by microscopic examination of stained stool smear by special stain. a- What is (are) the revealed causative parasite (s)? C. parvum, C. cyaetenensis, I. belli, Microsporidia. b- Name the type of stain used to reveal the causative parasite (s)? Modified Ziehl-Neelsen stain. c- If the parasite could be transmitted by autoinfection, what would be your diagnosis? C. parvum infection and may be I. belli infection. Case