COCCIDIAN PARASITES Dr Mohit Bhatia Assistant Professor Department

COCCIDIAN PARASITES Dr. Mohit Bhatia Assistant Professor Department of Microbiology AIIMS, Rishikesh

LAYOUT • INTRODUCTION TO COCCIDIA • CRYPTOSPORIDIUM SPECIES • CYCLOSPORA SPECIES • CYSTOISOSPORA SPECIES • MICROSPORIDIUM SPECIES

COCCIDIA Thick-walled oocysts excreted in feces In Humans • Cryptosporidium • Cyclospora • Isospora • Sarcocystis • Toxoplasma

Cryptosporidium, Cyclospora, and Cystoisospora • Secretory diarrhea without RBC or WBC in the stool. • None are easily found in routine “stool for ova and parasites. ” • Modified acid-fast staining is useful for all of the Coccidians. Isospora belli Cyclospora Cryptosporidium
 C. canis,")
Species of Cryptosporidium C. parvum C. hominis (previously C. parvum genotype 1) C. canis, C. felis, C. muris

Habitat of C. parvum • In the form of trophozoite. • It is present in the intestinal epithelial cell. • Remaining just within brush border.

MORPHOLOGY TROPHOZOITE OOCYST THICK WALLED THIN WALLED

Trophozoite • Measures 1 micro meter in diameter. • They are found on brush border (micro villous surface) of small intestine. • They grow into schizonts.

OOCYST These oocyts are either: • 1. Thickwalled-80% passed in feces THICKWALLED OOCYST • 2. Thin walled -20% excyst endogenously causing internal autoinfection • Oocyst contain 4 sporozoites. NO SPOROCYSTS PRESENT • Size - 4 -5µm THIN WALLED OOCYST

Modes of infection Reservoir host- Live stock, cats, dogs, birds etc. Portal of entry- occurs by ingestion of oocysts usually with • contaminated water • fecal-oral and • anal oral transmission from person to person Susceptibility- Veterinary personnel animal handlers are at high risk
 of C. parvum is only 132")
Transmission • The 50% infective dose (ID 50) of C. parvum is only 132 oocysts for healthy persons with no previous serological immunity to cryptosporidiosis

• Outbreaks result from drinking water of surface water sources -lakes and rivers. • Swimming pools and water park wave pools • Also, untreated groundwater or well water public drinking water supplies. • The highly environmentally resistant cyst of C. parvum survive various drinking water filtrations and chemical treatments such as chlorination. • Food can be contaminated by either an infected person or an asymptomatic carrier. The oocysts do not survive cooking, but food contamination can occur

Person-person transmission • Day-care centers, where infants or younger children are clustered within classrooms, share toilets and common play areas • Day-care employees through careless diaper-changing or through washing the laundry of infected children. • Nosocomial settings • Aerosol infection is fairly likely, since Cryptosporidium oocysts are shed in large numbers during acute infection and are immediately infective to others

Persons most likely to be infected by Cryptosporidium are: • Infants and younger children in day-care centers • Those whose drinking water is unfiltered and untreated • Involved in farming practices such as lambing, calving, and muck-spreading • Engaging in sexual practices that brings a person into oral contact with feces of an infected individual • Patients in a nosocomial setting with other infected patients or health-care employees • Veterinarians who come in contact with farm animals • Travelers to areas with untreated water • Living in densely populated urban areas • Owners of infected household pets (rare)
INTRA CELLULAR 2)EXTRA CYTOPLASMIC 3)PRESENT IN PARASITOPHOROUS VACUOLE")
MONOXENOUS LIFE CYCLE OF C. parvum 1)INTRA CELLULAR 2)EXTRA CYTOPLASMIC 3)PRESENT IN PARASITOPHOROUS VACUOLE
")
Life cycle of C. parvum(monoxenous)

Modes of infection

Clinical manifestations in immunocompetent Ø The incubation period - Two days - week. Ø In immunocompetent patients, it is an acute, yet self-limiting diarrheal illness (1 -2 week duration), and symptoms include : • Frequent, watery diarrhea • Nausea • Vomiting • Abdominal cramps • Low-grade fever

Immunocompromised persons CD 4 counts of <200 cell/cubic mm Ø The illness is much more severe Ø Debilitating, cholera-like diarrhea (up to 20 liters/day) • Severe abdominal cramps • Malaise • Low-grade fever • Weight loss • Anorexia

Detection and Diagnosis • Stool Conc. Technique: Formalin ethyl acetate • By a biopsy of intestinal tissue. -"patchy" nature of parasitic infection ): • The modified acid-fast stain is traditionally used to detect –oocysts(4. 2 -5. 4 um) have sporozoites (dd from Cyclospora-larger and unsporulated)

Cryptosporidium • 4 -5 mm oocysts • 4 sporozoites • no sporocysts Cyclospora • 8 -10 mm oocyts • 2 sporocysts • 2 sporozoites each Isospora belli • 30 x 12 mm oocyts • 2 sporocysts • 4 sporozoites each

OTHER DIAGNOSTIC METHODS • Anti-cryptosporidial Ig. M, Ig. G, and Ig. A can be detected by ELISA or by the antibody immunofluorescence assay (IFA), but neither of these assays can provide a direct diagnosis of cryptosporidiosis. • Recently, new genetic methods of detecting C. parvum have been developed, using PCR or other DNA-based detection methods.

TREATMENT • NITAZOXANIDE


Cyclospora cayetenisis • Cyclospora is associated with diarrhea. • 1990 - virtually unknown before about • 1996 -Contaminated Guatemalan raspberry, cause of a United States outbreak of Cyclospora in. • “yuppie disease”.
")
MORPHOLOGY • OOCYST DEFINATIVE HOST – HUMAN BEINGS (for Cyclospora cayetanensis)

• 8 -10 micro meter in diameter • Contains 2 sporocysts each containing 2 sporozoites • Sporozoite contain membrane bound nucleus and micronemes

Gametogony Oocyst Sporozoites penetrate epithelium Producing merozoites Invade other epithelial cell Excystation In small intestine Unsporulated Oocyst Passed in feces 7 -13 days mature oocyst(4 sporozoites) Human Infection Through Water(oocyst)


Modes of infection • Ingestion of contaminated food with sporulated oocyst. • Contaminated water • Contaminated raspberries. • Contaminated basil leaves.

Clinical disease • Acute infective diarrhea • Incubation period: 2 to 11 days Immuno competant individual: 1)Rapid onset of watery diarrhea 7 to 8 stools per day 2)Nausea, anorexia, abdominal cramps 3)Low grade fever and malaise 4)Self limiting remission in 3 -4 days followed by relapses from 4 -7 weeks Immuno compromised individual 1)Diarrhea is prolonged 8 -7 weeks and severe. 2)Biliary diseases have been reported

lab diagnosis Light microscopy Auto florescence Concentration methods
 sporocystic residuum(sr) Stieda body (st).")
Normal light miscroscopy. Three mature, living oocysts sporozoites (sp) sporocystic residuum(sr) Stieda body (st). Bar = 10 µm.
. • The outer wall is distinct")
Direct wet preparation with no staining (x 1650). • The outer wall is distinct and thick. • Each body contains several refractive granules. • 2 sporocysts in one oocyst

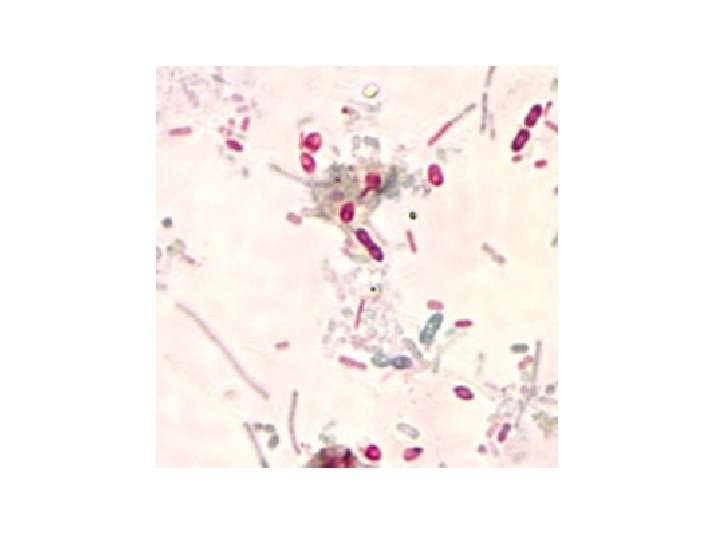
Cyclospora cyst taking zeihl neelson staining

AUTO FLUORESCENCE • Cyclospora organism flouresce when examined with an UV flourescent microscope. • This factor should be taken into consideration
,")
TREATMENT • Trimethoprim-sulfamethoxazole (TMP-SMX),

SEE WHETHER THE RASPBERRY ARE NOT CONTAMINATED BEFORE YOU EAT SEE THAT THE WATER IS NOT CONTAMINATED


Cystoisosopora belli • Apicomplexa • Coccidia • Monoxenous life cycle. • Coccida parasites are identified based on the structure of the oocyst.

• Sporulated oocyst is the infective stage • Invades intestinal epithelial cells • Often asymptomatic • Symptoms mild gastro-intestinal distress to severe dysentery • Often self-limiting, but can become chronic • Symptoms more severe in AIDS patients

• • HABITAT: Inside human beings. In form of trophozoites. Resides in epithelial cell of small Intestine Here schizogony and sporogony occurs

Morphology • OOCYST 2 types: Immature oocyst Mature oocyst DEFINATIVE HOST – HUMAN BEINGS

Immature oocyst: • Size- 15µm× 20µm • Shape – rugby ball • Develop inside epithelial cell of small intestine. • Central individual mass of protoplasm. • They are unsporulated. • They are shed in feces Immature oocyst

Mature oocyst • Size – 20µm × 10µm • Shape- rugby shape It is elongated and narrow at one pole with neck like restricted area. • 2 sporocyst with 4 sporozoites each Mature oocyst

Modes of infection • Reservoir host: NIL • Source : contaminated food and water. • Portal of entry: ingestion of oocyst

Infection by Oocyst Gametogony, Fertilisation oocyst Merozoites Undergo Schizogony In epithelial cell Sporocyst Invade epithelium Of small intestine-trophozoite Trophozoite Undergo schizogony

CYSTOISOSPORA BELLI LIFE CYCLE

Clinical disease • Acute infective diarrhea • Incubation period: 2 to 11 days immunocompetant individual: 1) Rapid onset of watery diarrhea 7 to 8 stools per day 2) Nausea, anorexia, abdominal cramps 3) Low grade fever and malaise 4) Self limiting remission in 3 -4 days followed by relapses from 4 -7 weeks Immuno compromised individual 1)Diarrhea is prolonged 8 -7 weeks and severe. 2)Biliary diseases have been reported
 DUODENAL ASPIRATE BIOPSY")
LAB DIAGNOSIS DIRECT MICROSCOPY (FAECES) DUODENAL ASPIRATE BIOPSY

Diagnosis-Mod acid fast staining Autofluorescence Biopsy of Intestinal mucosa PCR 20 -33 um x 10 -19 um
 • Pyrimethamine with folinic acid in allergic individuals • Ciprofloxacin-")
TREATMENT • Trimethoprim-sulfamethoxazole (TMP-SMX) • Pyrimethamine with folinic acid in allergic individuals • Ciprofloxacin- 2 nd line drug

PREVENTION Wash food such as green salads and fruits, especially if it is to be eaten uncooked. WASH YOUR HANDS BEFORE YOU EAT YOUR FOOD Eat meat only when it is cooked to "well done". For example, do not eat meat tartare or "rare" meat.

MICROSPORIDIOSIS

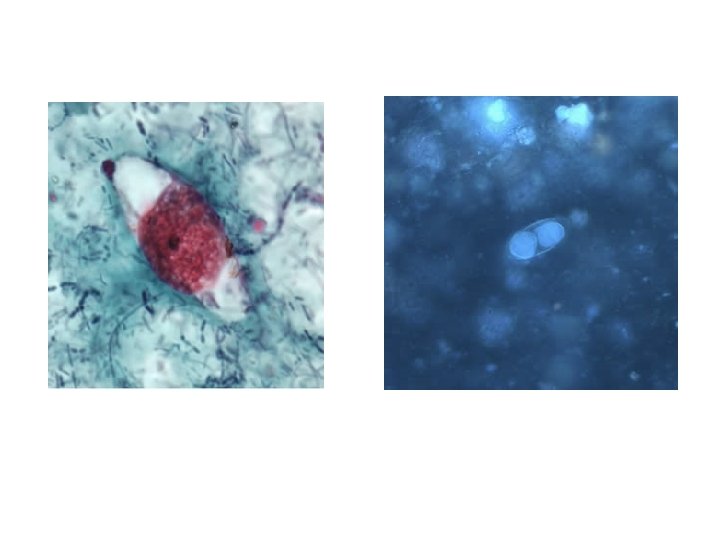
DIAGNOSIS • MICROSCOPY: Chromotrope 2 R, Quick-Hot Gram Chromotrope technique, Calcofluor white • IFA • MOLECULAR METHODS

TREATMENT • Albendazole is the drug of choice for ocular, intestinal, and disseminated microsporidiosis. • Topical fumagillin is used to treat microsporidial keratoconjunctivitis.

- Slides: 59