Odessa national medical university Department of Anesthesiology Intensive










 Pa. CO 2")





 n Normal shunting: (2~3 % of CO)")

 n Vascular obstruction n Pulmonary embolism n")





,")













 or")



- Slides: 52
Odessa national medical university Department of Anesthesiology, Intensive Care and Emergency medicine Intensive therapy of acute respiratory insufficiency (failure)
Transfer of oxygen of inhaled air into the blood and of waste carbon dioxide of blood into the lungs Ventilation Gas Exchange Hypoxemic respiratory failure Hypercapnic respiratory failure
Respiratory insufficiency inadequate blood oxygenation or CO 2 removal A syndrome rather than a disease Pa. O 2 < 60 mm. Hg or Pa. CO 2 > 50 mm. Hg Hypoxemic Pa. O 2 < 55~60 mm. Hg or Sa. O 2 < 90% with Fi. O 2 >= 60% Hypercapnic Pa. CO 2 > 45~50 mm. Hg This two types of respiratory failure always coexist Acute: develops in minutes to hours, p. H < 7. 30 Chronic: develops over several days or longer
Ventilation CNS Efferents CNS Afferents/ Intergration Chemoreceptors Respiratory Muscles Chest Wall PNS Disfunction of any component of the ventilation system may result in ventilatory failure Pa. O 2 Pa. CO 2 Alveolar Ventilation Airways Alveoli Minute Ventilation
Control of Ventilation Mechanical stimuli, Chemical stimuli, Higher CNS input Medulla Dorsal respiratory group Ventral respiratory group Pneumotaxic center Dorsolateral pons Nucleus parabrachialis medialis Ventral and Lateral columns of the spinal cord Phrenic n. diaphragm Intercostal n. intercostal m. Switching between the inspiratory and expiratory phase rhythm, rate, depth of breathing
Chemical Stimuli n Peripheral chemoreceptors n Carotid bodies, Aortic bodies n Stimulus: Pa. O 2, Acidemia (p. H), Pa. CO 2 n Central chemoreceptors n Near the ventrolateral surface of the medulla n Stimulus: H+ of brain liqvor (p. H), Pa. CO 2
Chemical Stimuli n Hypoxia peripheral receptors n Hypercapnea central receptors n For the same p. H change, the ventilatory response to respiratory acidosis is greater than metabolic acidosis: n CO 2 (gas) readily crosses the blood-brain barrier, but H+ and HCO 3 - (ion) cross the blood-brain barrier more slowly.
Respiratory Muscles n Inspiration: active n Diaphragm: n n Intercostal muscles: n n phrenic n. (C 3 -5) T (their own level) Accessory muscles n Expiration: passive n A bdominal muscles: (active expiration) n n Lower T and L level Intercostal muscles: n T (their own level)
O 2 demand CO 2 production Dead space Respiratory drive Motor neuron/nerve function Muscle strength Respiratory mechanics VE MSV Minute Ventilation Maximal Sustainable Ventilation Pa. CO 2 = K · VCO 2 / VA VA= VE (1 - VD/VT) VT-tidal volume VD-dead space ventilation VA –alveolar ventilation Ventilatory Demand MSV = MVV/2 MVV = 40 FEV 1 MVV: Maximal voluntary ventilation Ventilatory Supply Ventilaroty Demand > Ventilatory Supply Ventilatory Insufficienty
Respiratory Insufficiency in a patient with Asthma Ventilatory Demand Ventilatory Supply
Dead Space Ratio CO 2 Production VA= VE (1 - VD/VT) Pa. CO 2 = K · VCO 2 / VA ↑CO 2 Production ↑Dead Space Ratio ↓Minute Ventilation Hypercapnic Respiratory Insufficiency
Hypercapnic Respiratory Insufficiency Increase carbon dioxide production n Fever, sepsis, seizure, obesity, anxiety n Increase work of breath (Asthma, chronic obstructive pulmonary desease (COPD)) n High carbohydrate diet with underlying lung disease (high RQ (respiratory quotient) )
Hypercapnic Respiratory Insufficiency Decreased minute ventilation n CNS disorders n stroke, brain tumor, spinal cord lesions, drug overdose n Peripheral nerve disease n Guillain-Barre syndrome, botulism, myasthenia gravis n Muscle disorders n muscular dystrophy, respiratory muscles fatigue n Chest wall abnormalities n scoliosis, kyphosis, obesity n Metabolic abnormalities n myxedema, hypokalemia n Airway obstruction n Upper airway obstruction, Asthma, COPD
Hypercapnic Respiratory Failure Increase dead space n Airway obstruction n Upper airway obstruction n Asthma, COPD n Foreign body aspiration (check-valve) n ARDS (acute respiratory distress syndrome), Pulmonary embolism n Chest wall disorder
PAO 2 = Pi. O 2 – PACO 2/RQ A-a gradient = PAO 2 – Pa. O 2 Response well to oxygen therapy Pa. O 2 = [ Fi. O 2(PATM-PH 2 O) –Pa. CO 2/RQ] –[ A-a gradient] Low Inspired Oxygen Alveolar Hypoventilation Shunt V-Q(ventilation/perfusion) mismatch Diffusion impairment Hypoxemic Respiratory Failure
Hypoxic Respiratory Failure 1. Low inspired oxygen n High altitudes 2. Hypoventilation n Conditions described in hypercapnic respiratory failure n Oxygen therapy improve hypoxemia but may worsen the hypoventilation
Hypoxic Respiratory Failure 3. Shunt (right-to-left shunt) n Normal shunting: (2~3 % of CO) n Some of the bronchial arterial blood n Some of the coronary venous blood n Abnormal shunting: n Congenital defects in the heart or vessels n Lung atelectasis or consolidation n Pneumonia, Cardiogenic or Non-cardiogenic pulmonary edema n Resistant to O 2 supply when shunt fraction of CO > 3 0 % n Hypercapnia develops when shunt fraction > 6 0 %
Example: Shunt Fraction of 50% with Pi. O 2=150 mm. Hg Ca. O 2= (20+15)/2 = 17. 5 Pa. O 2 = 54% Sa. O 2= (100%+75%)= 87. 5% Pa. O 2 = 54% Resistant to 100% oxygen
Hypoxic Respiratory Failure 4. Ventilation-Perfusion Mismatch (V-Q) n Vascular obstruction n Pulmonary embolism n Air-space consolidation n Pneumonia, Pulmonary edema
Hypoxic Respiratory Failure 5. Diffusion Impairment n Interstitial lung disease n Pulmonary fibrosis, Connective tissue disease, Interstitial pneumonia, interstitial pulmonary edema n ARDS. RDS n Obstructive lung disease n Emphysema, Asthma
The capillary transit time of RBC is 0. 75 seconds. With normal DL (diffusion level), it takes < 0. 25 seconds to equilibration. Only when the DL is severely limited (<0. 25 normal) or the transit time is markedly shorten (<0. 25 seconds) is it possible to have a Pa. O 2 less than PAO 2.
Approaching a Patient with Respiratory Failure
History & Physical Examination n Acute or Chronic n Underlying ( heart / lung ) diseases n Drugs history n Wheezing? Rhonchus? Diminish breath sound? Air-space consolidation? n Symptoms of heart failure n Clubbing finger
Clinical Presentations of Acute Respiratory Failure n B reath pattern: n rapid-deep rapid-shallow slow-shallow n Accessory respiratory muscles used: n Paradoxical respiration: n Hypoxemia n dizziness, irritable, conscious change, tachycardia, cyanosis, peripheral vasodilatation, pulmonary vasoconstrition. n Hypercapnia n Headache, somnolence, conscious change
Workup n LAB: n Arterial blood gas; Pulse oxymeter n complete blood count (CBC), differential count (DC), Creactive protein n Cardiac enzyme n Electrolytes: K, Pi, Mg… Ca, Na…. n B iochemistry data, n EKG (cardiac echo) n Chest X-ray (chest CT, lung scan) n Lung function test n Pulmonary artery catheter n Neurological exam (Brain CT, EEG……)
Dyspnea n Short of breath n Abnormally uncomfortable awareness of breathing subjectively n Increased work of breath n
Dyspnea of rapid onset
Dyspnea of slow onset
Dyspnea with associated symptoms
Treatment
A…B… C n Establish Airway n Establish Ventilation n Oxygen Therapy n Treat the circulatory failure n Oxygen delivery = {(Sa. O 2·Hb· 1. 3 9) + (0. 0 0 3 ·Pa. O 2)} X Cardiac Output
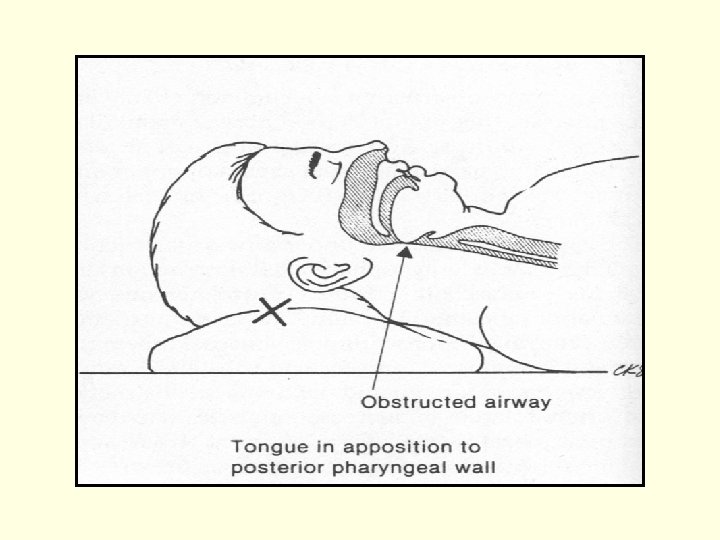
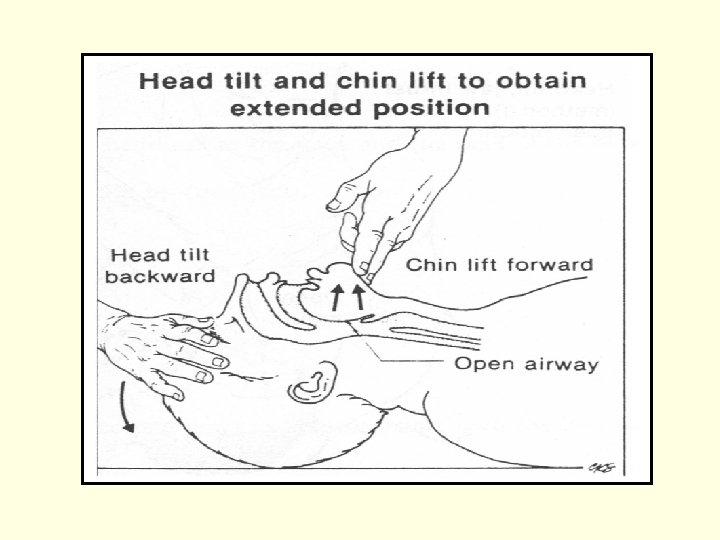
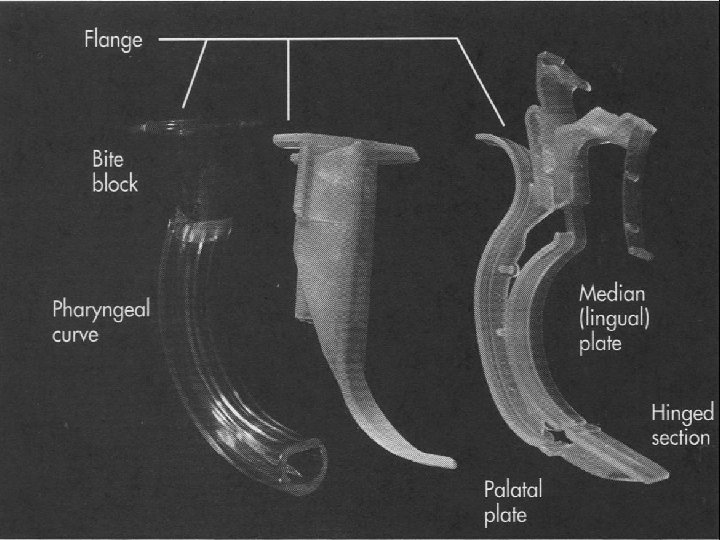
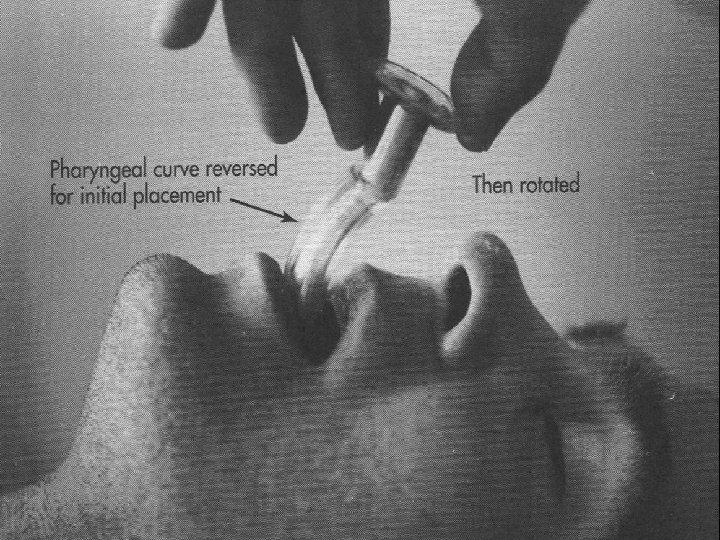
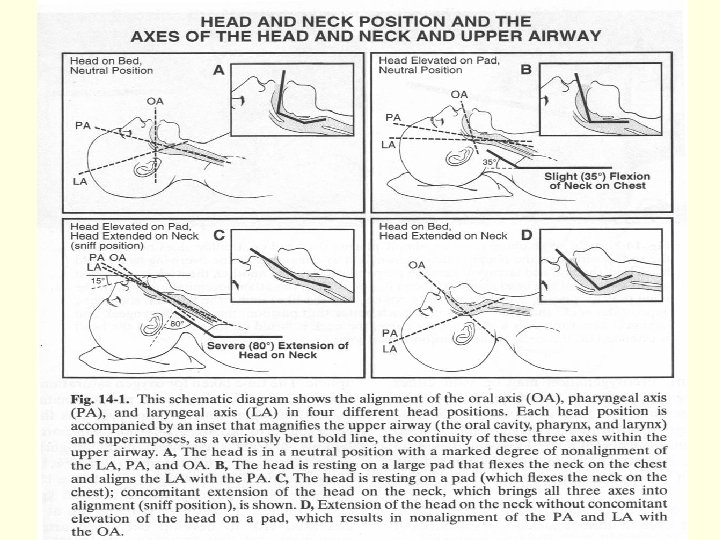
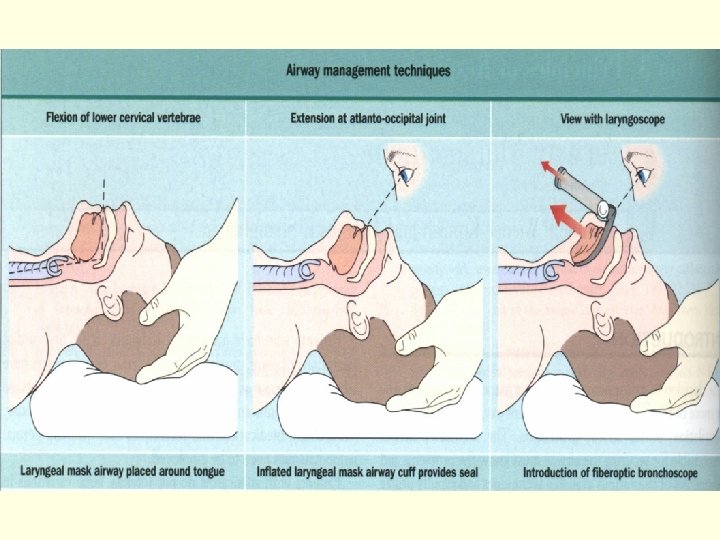
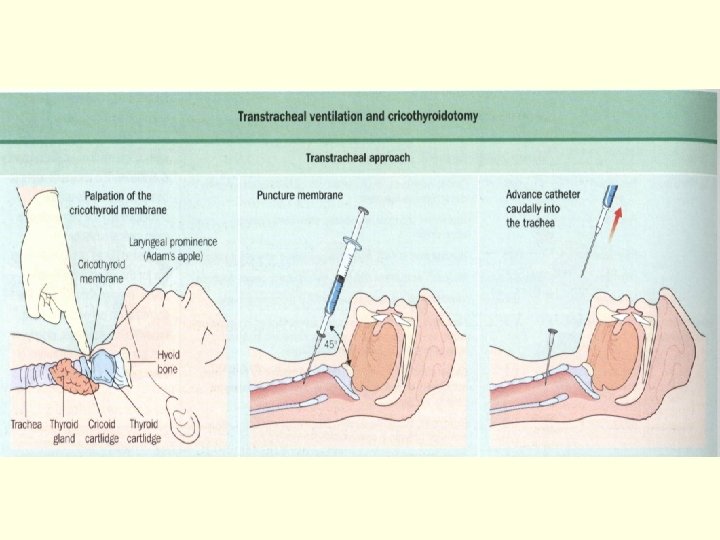
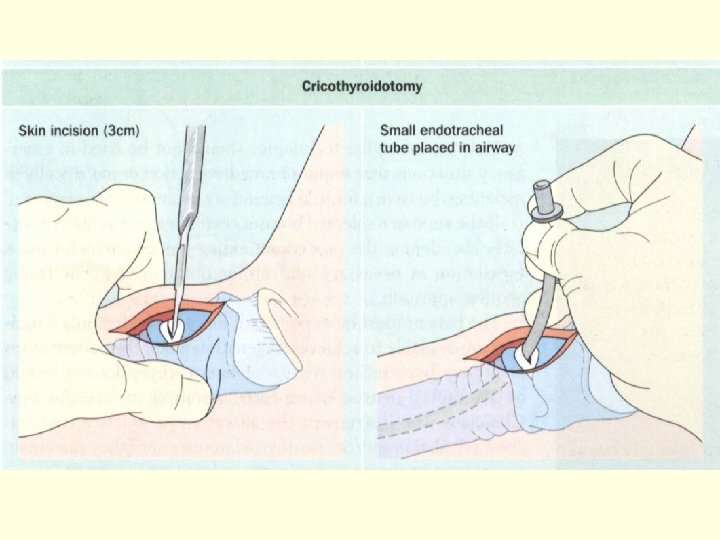
Airway Management n Head tilt-chin lift / Jaw-thrust maneuver n Artificial airway (Oral or Nasal airway) n Laryngeal Mask Airway n Endo-Tracheal intubation n Emergent Cricothyroidotomy n Tracheostomy
LMA
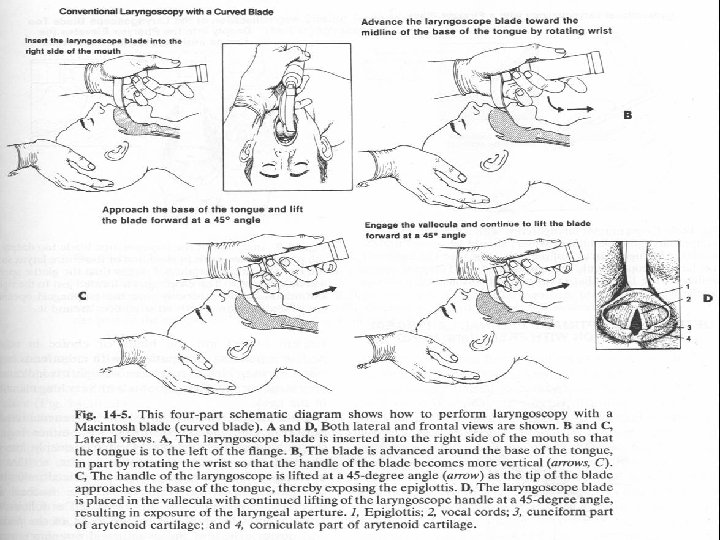
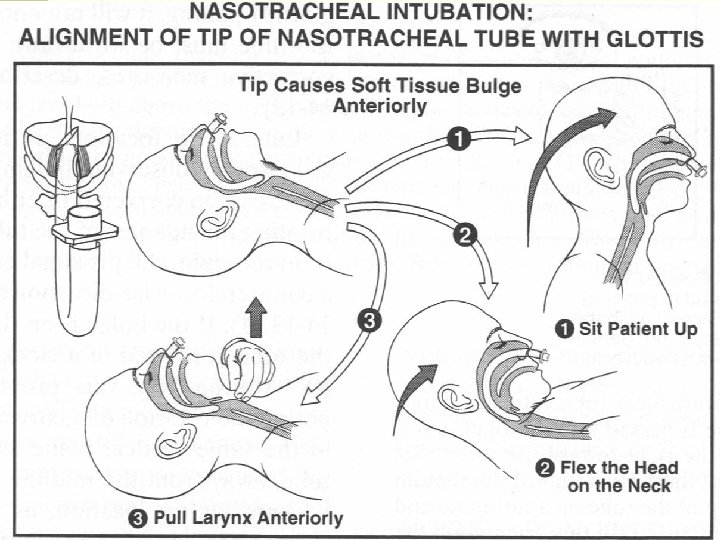
Endotracheal intubation n Direct oratracheal intubation n B lind nasotracheal intubation n Flexible fiberoptically guided intubation
Reasons for E-T intubation n Establish Airway n Airway Protection: Prevention of aspiration and allowing for the suction of pulmonary secretions n Initiation of Mechanical Ventilation: for respiratory failure n Hyperventilation for IICP (increased intracranial pressure ): keep Pa. CO 2 around 30 mm. Hg
Sellick Maneuver
Oxygen therapy Low Flow High Flow n Nasal cannula n Venturi n Simple mask n All-purpose n Partial rebreath mask n T-piece n Non-rebreath mask
Mechanical Ventilation n NIPPV Non-invasive Positive Pressure Ventilation n CPAP(continuous positive airway pressure) or Bi. PAP (bilevel positive airway pressure) COPD, CHF Contraindication n Conventional Mechanical Ventilation n Volume control, Pressure control (Assist-Control) SIMV (Synchronized Intermittent Mandatory Ventilation) n Pressure support n
Mechanical Ventilation n Adequate oxygenation n Pa. O 2 > 6 0 mm. Hg or Sa. O 2 > 9 0 % n Optimal ventilation (Pa. CO 2) n Permissive hypercapnea for ARDS and Obstructive lung diseases n p. H is more important; consider giving bicarbonate for p. H less than 7. 2 n Hyperventilation for IICP n Rest the respiratory muscles of patients
Mechanical Ventilation n Patient-Ventilator Synchrony n Ventilator mode and setting, sedation/paralysis n Respiratory Rate < 3 5 /min n Fi. O 2 < 60 % (use PEEP and I/E ratio) n Plateau Pressure < 3 0 ~ 3 5 cm. H 2 O Peak Airway Pressure < 5 0 cm. H 2 O n Use PEEP n Avoid Air-trapping / Auto-PEEP
Thank you for your attention!!!