Neurointensivists Role in Neurosurgical Care Training Lori A









")
















- Slides: 27
Neurointensivist’s Role in Neurosurgical Care & Training Lori A. Shutter, MD Director, NSICU/Neurocritical Program Assoc. Professor of Neurosurgery, Neurology & PMR University of Cincinnati Medical Center
Objectives q Describe the specialty of neurocritical care. q Review the requirements for certification in neurocritical care. q Discuss the role of a neurointensivist in neurosurgical residency training.
Modern Intensive Care q “Intensive-care medicine has become the art of managing extreme complexity—and a test of whether such complexity can, in fact, be humanly mastered. ” Atul Gawande, The New Yorker, 1/6/08 q Bundles; Check lists; Time Outs q Protocols; Guidelines; Evidence-based Care q Multidisciplinary; Collaborative q JACHO; CMS
What is a Neuro-intensivist? q A physician devoted to comprehensive multisystem care of the critically ill neurological patient. Assumes a primary care role for patients in the ICU, coordinating both neurological & medical management. q Has a unique concern with the interface between the brain and other organ systems in the setting of critical illness. q Takes on responsibility for various elements of ICU care that might otherwise be provided by multiple subspecialists (i. e. cardiology, endocrinology, infectious diseases, pulmonary medicine, and neurology). q Proficiency with standard ICU monitoring, as well as specialized neuro-monitoring and interventions. q
Are Neurointensivists Needed? q Disclosure: I am biased on this topic q Advances in the treatment of neurological conditions Advances in critical care Uniqueness of the neurological patient Increased patient / family awareness Collaboration for professional & academic growth Multi-disciplinary team care q q q
History of NCC q Neurological Intensive Care AAN course ’ 80 – 87 q q Gap from ’ 88 – 99, restarted in 2000 Subspecialty development: late ’ 80 s – early 90 s MGH: Allan Ropper q Columbia: Matt Fink q Hopkins: Dan Hanley and Cecil Borel q UVa: Tom Bleck q q Growth through Neurology departments, or other intensivists in units with high neurosurgical volumes q Focus changed to Neurocritical Care, NOT specialized stroke units
Organized NCC q Organized NCC has made major strides in last decade AAN CCEN Section* q Neurocritical Care Society* q SNACC* q AANS/CNS Joint Section on Neurotrauma & Critical Care q German Neurocritical Care Working Group q q Neurocritical Care Society 2007 saw the 5 th Annual Meeting q 651 physician members (105 residents); 774 total members q q NCC recognized as a subspecialty by UCNS* in 2006
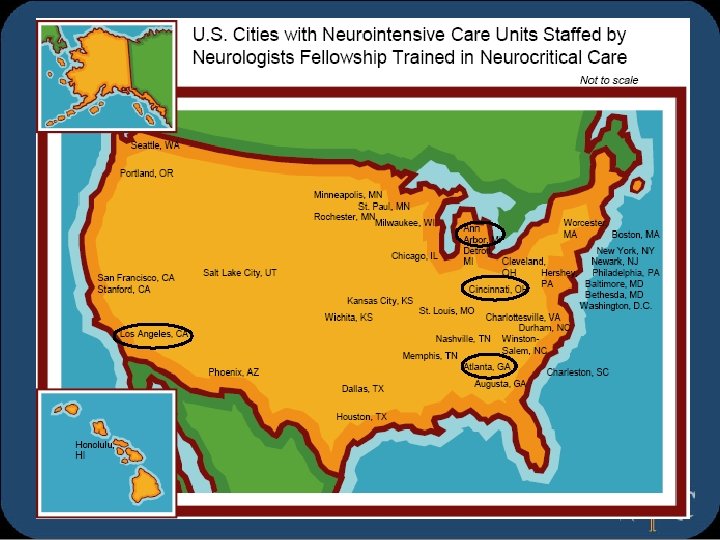
Neurocritical Care q Dedicated Neuro-ICUs with fellowship trained neurointensivists in the US = 50* q q 29 states; 39 cities & DC NCC Program Models Division of Neurology vs Neurosurgery vs Anesthesiology q Department of Critical Care – Multidisciplinary q q Neuro-ICU models Closed vs ‘Semi-closed’ vs Open q Primary providers vs Co-attendings vs Consultants q
Neurocritical Care Certification q q First certification exam in NCC in 12/07 Eligibility for exam: fellowship or practice tracts. Fellowship tract: documentation of training in an accredited NCC fellowship program q Practice tract available until 2012 q q Exam components Neurological – 48% q General medical critical care – 47% q Procedural – 5% q q Current diplomates in NCC = 91. q Next examination – 12/08
Neurocritical Care Training q Fellowship Training Programs 39 in the US (in 18 states) q < 25 currently active q 2 year training curriculum developed based on UCNS / ACGME guidelines q Program accreditation through UCNS starting in 2007. 11 programs submitted applications. q q Specialties eligible for training in NCC: neurology, neurosurgery, emergency medicine, anesthesia, internal medicine, pediatrics
NCC Training Requirements q Duration of training 12 months of ICU experience q > 50% focusing on primarily neurological & neurosurgical conditions q Recommend 18 – 24 months to provide adequate elective & off-service time q q Additional qualifications q q Provider / instructor in ACLS, ATLS, PALS, FCCS Faculty Provide direct supervision in ICU q Demonstrate adequate training / experience in NCC q Minimum of 25% of time dedicated to NCC q
Neurological Conditions q q q q Cerebrovascular Neurotrauma Seizures Neuromuscular diseases Neuro-oncology Infections Toxic-metabolic Inflammation / demyelination q q q q Encephalopathies Movement disorders Neuroendocrine Clinical syndromes Peri-operative neurosurgical care Neurorehabilitation Pharmacotherapeutics
EEG box ICP monitor Pbt. O 2 Feeding Tube ET Tube CVL EEG leads
Tube feed pump EEG Monitor Ventilator IV Pumps Pbt. O 2
General Medical Conditions Cardiovascular q Shock / resuscitation q Coronary Ischemia q Neurogenic Cardiac Abnormalities q Cardiac Arrhythmias q Hypertensive Crisis q Pulmonary edema: cardiogenic & non-cardiogenic q Pulmonary embolism q Acute aortic / peripheral vascular disorders q Advanced cardiovascular monitoring & derived parameters
General Medical Conditions Pulmonary q Respiratory failure q Pneumonitis / pneumonia q Adult Respiratory Distress Syndrome q Upper airway obstruction q COPD / asthma q Neurogenic breathing patterns q Mechanical ventilation: modes, weaning, monitoring q Pleural diseases: empyema, effusion q Pulmonary hemorrhage / hemoptysis q Sleep apnea
General Medical Conditions Renal q Fluids / electrolytes q Acute Renal Failure q q q Drug dosing Acid-base disorders Hemodialysis Rhabdomyolysis UTI / Urosepsis GI q GI bleed q GI perforation q Ileus q Obstruction q Hepatic failure q Pancreatitis
General Medical Conditions Metabolic/ Endocrine q Nutrition q Thyroid function q Adrenal crisis q Diabetes q Pheochromocytoma q Systemic Inflammatory Response Syndrome q Fever/thermoregulation Infectious q Antibiotics q Drug resistance q Hospital acquired infections q AIDS q Central fever
General Medical Conditions Hematologic q Hemostasis defects & therapy q Blood component rx q Hemolytic disorders q Hypercoagulable states q DVT prophylaxis q Anticoagulation q Transfusion reactions q q q q Immunology Transplantation General Trauma Burn management ICU Agitation Monitoring Prognostication
Procedural Competencies q q q Arterial catheters Central venous catheters Pulmonary artery catheters Management of vasoactive medications Airway Management Non-intubated q Direct laryngoscopy q Endotracheal intubation q Mechanical ventilation q CPAP/Bi. PAP ventilation q q q Interpretation of bedside pulmonary function CPR/ACLS (with certification)
Procedural Competencies q q q Lumbar puncture; Shunt / ventricular drain tap Conscious sedation & barbiturate anesthesia Neuro-monitoring ICP, CPP, Pbt. O 2, Sjv. O 2 management q Management of EVDs q TCDs q EEGs q q q Management of plasmapheresis & IVIG IV & intraventricular thrombolysis Interpretation of neuroimaging studies Moderate hypothermia
Training Residents in NCC q Work hour restrictions have damaged the ICU experience for residents Attitude change – from physicians to shift workers q They are less involved and many are less happy q Frequent transfers to other services rather than managing the problems q Attendings aren’t reading sleep deprivation literature because we are doing the resident’s work! q q PGY-1 s (neurosurgery, neurology, others) have been added to the ICU rotation q BUT – even the best ones have trouble being alone in an ICU that early
Training Residents in NCC q Neurotrauma / Critical Care Fellowships q q It will not meet criteria for NCC Certification q q Is this adequate critical care training? Does that matter? That Depends Are you managing anything other than trauma? Do you want to? q Does it provide adequate exposure to medical critical care? q What are you going to focus on for your career? q Do you want extra certifications? q
Training Residents in NCC q I don’t have the answer q Exposure to the specialty q Division of Neurosurgery q Collaboration q Interwoven in didactic / conference sessions q Dedicated ICU time q Not just 30 minutes on am rounds! q PGY-1 year q As part of neurology requirement q Advanced training / Enfolded ‘fellowship’
What to do? q Develop connections with NCC organizations q Work with NCS leadership to address issues specific to neurosurgical training q Decide if NCC should be a focus of your program q Develop a curriculum with your neurointensivist q Based on fellowship training requirements
Thank You