Interesting Case Conference 2212014 Raina Flores Adam Johnson














: O Rh(D)")
 • Occurs when maternal plasma contains")
 negative")

 negative women")
 negative women")







 in all")




")
- Slides: 35
Interesting Case Conference 2/21/2014 Raina Flores, Adam Johnson
Case 1 • On 4/28/2009, patient RD received cryoprecipitate from Donor X • Donor X – 12/29/13: HIV first documented – Last negative donation: 3/11/09 – Number of negative donations since 3/09: 0 • Patient RD: – 51 year old man – PMH: LVAD (2009) – 10/14/2008: HIV 1 & 2, non-reactive
FDA Lookback Requirements Within 3 days of donor HIV positivity, all records of previous donations must be reviewed, to include: • All donations 12 months prior to last negative donation or NAT/p 24 antigen/serologic testing • Donations must be quarantined, with exception to those using validated viral clearance procedures – All facilities in which donations were shipped (consignees) must be notified. Same quarantine applies. • Supplemental testing for HIV must be performed on the reactive donation – You must notify consignees of results • Within 12 weeks of positive supplemental, or positive screen but supplemental tests unavailable, you must notify recipients/recipient physicians and recommened HIV testing – If recipient a minor, deceased, adjudged incompetent by a State court, or if recipient competent but state law allows for disclosure, a relative or legal representative must be notified
Current Status • 2/1/2014: HIV 1 & 2, non-reactive • It is very unlikely the patient will become HIV+ from the transfusion in 2009
Background • 1982: 1 st year HIV transmission was documented as a result of transfusion • Risk of HIV transmission from transfusion: - 1983: ~1/100 (San Francisco) - 2008: 1/1. 5 M - Current: 1/2 M • Donor screening • Lab screening HIV Transmission Through Transfusion — Missouri and Colorado, 2008. Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report, October 22, 2010.
Case Report • In 2008, a man donated blood that was screened positive for HIV • This man had given blood in the past – Donation questionairre: denied HIV-related inquiries – 6/2008: whole blood donation screened negative for HIV by enzyme immunoassay (EIA) and nucleic acid amplification testing minipools of plasma specimens (MP-NAT) – 11/2008: donation tested positive for HIV by EIA, MP-NAT, and indirect immunofluorescence assay HIV Transmission Through Transfusion — Missouri and Colorado, 2008. Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report, October 22, 2010.
Recipient A: • One died shortly after RBC/FFP transfusion due to complications of cardiac disease
Recipient B: • Screened HIV negative in 2005, denied HIV risk factors or blood transfusion since • 8/2008: kidney transplant; donor kidney tested HIV negative – • • 12/2008: serum nonreactive by EIA; plasma HIV RNA viral load 7, 240 copies/m. L; ↓↓ CD 4 cell count (48 cells/μL) Transplant rejection medication: mycophenolic acid – • Recieved FFP from 8/2008 donation Potent inhibitor of both lymphocyte proliferation and HIV replication in CD 4+ T cells and macrophages HIV DNA >99% indentical between recipient B and donor
Donor Re-examination • In April 2009, he agreed to a brief interview/HIV test – This test was reactive and confirmed by Western blot – The donor admitted to infidelity (male and female) while intoxicated, prior to his first donation
How could the donor infect recipient B if their HIV screen was negative at donation?
HIV: Eclipse Period • HIV screening: – NAT: 10 -15 days – Serologic: 22 days • Eclipse: interval between infection and development of detectable HIV RNA in plasma
FDA Required Screening • Questionnaire: – Permanent deferral: • History of HIV, clinical (IVDA, prostitution) or lab evidence – 12 -month deferral: • Skin penetration by non-sterile (non-donor contaminated) needle/instrument • Sex with HIV+/HIV high risk person (IVDA, M 2 M sex, prostitute) • >72 hour incarceration • Successfully treated syphilis/gonorrhea • Within 12 months, history of sex with prostitute/nonprescription drug user/hepatitis+ individual/practicing homosexual male (females only), all from date of last encounter
Incidence Report of transfusion-transmitted HIV infection may be underestimated by: 1. Recipient death before detection of HIV 2. Poor recall by infected recipients regarding transfusion history 3. Inability to confirm or rule out transfusion as the source of infection because no HIV-infected donors were identified 4. Underrecognition of HIV infections among recipients of potentially infected blood who recover from infection 5. Inappropriately attributing infection to lifestyle (e. g. , male-to-male sexual contact or injection drug use) HIV Transmission Through Transfusion — Missouri and Colorado, 2008. Centers for Disease Control and Prevention. Morbidity and Mortality Weekly Report, October 22, 2010.
Comments?
Case 2 • • 29 y/o G 2 P 1 6/10/2013 (OSH): O Rh(D) negative with negative antibody screen 11/6/2013 (OSH): anti-D identified on antibody screen (titer of 1: 64) 12/17/2013 (OSH): – Scanned note states that Rh. IG was given on 11/6/2013 – Also of note: "Pt. states she had Rhogam inj. @ MFM on 10/23/13“ • 1/23/2014 (VUMC): – Baby is born! • Hgb: 12. 3 gm/d. L PCV: 39% – DAT performed on cord blood sample is positive for Ig. G (4+) • 1/25/2014 (VUMC): – Hgb: 10. 6 gm/d. L PCV: 32% Reti. Ct: 10. 4 TBil: 16. 6 mg/d. L (up from 8. 1 mg/d. L on 1/24/2014) – Anti-D titers performed on maternal and baby cord blood samples • Mom’s anti-D titer = 1: 256 • Baby’s anti-D titer = 1: 64 – Rh. IG subsequently administered to mom
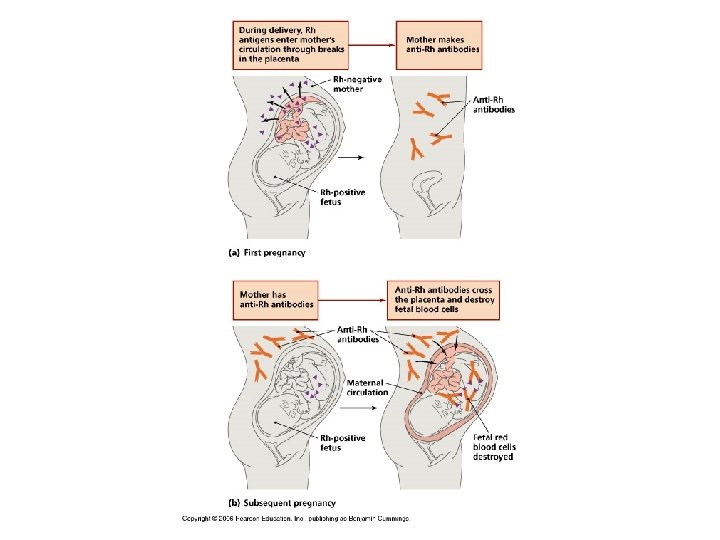
Hemolytic Disease of the Fetus and Newborn (HDFN) • Occurs when maternal plasma contains alloantibodies to antigens present on fetal RBCs – Fetal RBC destruction by spleen leads to anemia • • Severity of HDFN depends on antibody specificity, antibody titer, immunoglobulin class, and number of antigen sites on fetal RBCs Anti-D is most common cause of severe HDFN – Anti-c and anti-K also have high likelihood of severe HDFN • Rh(D) negative mother develops Ig. G antibodies D antigen exposed to fetal RBCs
Anti-D Immune Globulin • Before Rh. IG, 16% rate of alloimmunization of Rh(D) negative women during second pregnancy with Rh(D) positive child • Anti-D Ig. G antibody manufactured from human plasma – Pooled source from persons with high antibody titers to RBCs with Rh(D) antigen • Rho. GAM: – Preparation = “Cohn cold ethanol fractionation followed by viralclearance ultrafiltration” – Intramuscular administration • Rhophylac: – Preparation = ion-exchange chromatography isolation – Improved purity compared to Rho. GAM – Intravenous administration Am J Obstet Gynecol. 1985; 151(3): 289; Cochrane Database Syst Rev 2013; 1: CD 007885
Anti-D Immune Globulin • 300 microgram dose of Rh. IG contains enough anti-D to suppress the immune response to 15 m. L of Rh(D) positive RBCs (30 m. L Rh(D) positive whole blood) • Elimination half life = 30. 9 days • Anti-D titers are detected in maternal serum for several weeks – Titer usually <1: 4 – Concern for HDFN arises when titer reaches 1: 32 • At birth, baby may have +DAT – If double dose Rh. IG administration, up to 20% of babies may have +DAT – Strength usually 1+ or 2+ Arch Dis Child Fetal Neonatal Ed. 2001; 84: F 60 -2 Modern Blood Banking and Transfusion Practices. 2005; pp. 383– 395 Technical manual. 16 th ed. Bethesda, MD: AABB; 2008
Guidelines For Use of Anti-D Immune Globulin • Antepartum: – All Rh(D) negative women should receive antibody screen at first prenatal appointment for each pregnancy – At 28 weeks: • Second antibody screen (according to AABB) • Administer single dose of 300 micrograms of Rh. IG – Rate of alloimmunization of 0. 1% – Second antepartum dose? ? • May be given if patient has not delivered within 12 3/7 weeks of first Rh. IG dose • No current consensus Transfus Med Rev. 1988; 2(3): 129
Guidelines For Use of Anti-D Immune Globulin • Additional indications in Rh(D) negative women with potential Rh(D) positive fetus: – – Spontaneous or induced abortion Threatened abortion Ectopic pregnancy Invasive procedures: • Amniocentesis (16 to 22 weeks), CVS (10 to 12 weeks), fetal blood sampling – Partial mole – Intrauterine fetal demise (2 nd and 3 rd trimester) – Antepartum hemorrhage (2 nd or 3 rd trimester) • Placental abruption • Placenta previa • Blunt force trauma to abdomen
Guidelines For Use of Anti-D Immune Globulin • Postpartum: – 300 micrograms of Rh. IG within 72 hours of delivery of an Rh(D)-positive infant – Fetal maternal hemorrhage (FMH) is usually <5 m. L – >30 m. L occurs in 1 in every 200 to 300 deliveries • May need to give additional dose(s) of Rh. IG!!! Transfusion. 2012 Sep; 52(9): 1977 -82.
Evaluation of Fetomaternal Hemorrhage • Rosette test: – Exogenous anti-D antibodies added to maternal blood – Antibodies adhere to fetal Rh(D) positive RBCs – Additional Rh(D) positive “indicator cells” added, forming rosettes around fetal RBCs coated with anti-D Ig. G
Evaluation of Fetomaternal Hemorrhage • Kleihauer-Betke: – Smear of maternal venous blood is immersed in fixative, incubated in acid solution, and stained with erythrosine B – Acid elutes Hb. A, but Hb. F is resistant to acid elution – Hb. F RBCs are cherry red and Hb. A RBCs are uncolored (ghost cells) – Count 2, 000 RBCs, and determine % fetal RBCs – Rhophylac dose = (TBV x %fetal cells)/ 30 m. L http: //tulane. edu/som/departments/pathology
Evaluation of Fetomaternal Hemorrhage • Flow cytometry: – Quantifies the number of fetal RBCs by measuring the fluorescence intensity of monoclonal antibodies to Hb. F – Volume of fetal RBCs = %fetal RBCs x 50 • 50 represents the average maternal blood volume of 5 liters – Rhopylac dose = fetal RBC volume / 30 m. L – According to AABB standard: • If fractional dose <0. 5, then round down and add one dose • If fractional dose >0. 5, then round up and add one dose
Back to the patient • Alloimmunization vs. passive Rh. IG? ? – Mom’s anti-D titer (1: 256) higher than expected with Rh. IG administration alone – Cord blood DAT (4+) higher than expected with Rh. IG administration alone • Rh. IG failure? – Mom was alloimmunized but anti-D was not detected on initial antibody screen – Rh(D) alloimmunization occurred before Rh. IG was administered – Rh. IG dosage was not sufficient to provide “coverage” for large fetomaternal hemorrhage
Comments?
Case 3 • • 63 year old male PMH: Parkinson's disease Presented to VUMC on 2/8/2014 for reported weakness Labs: – – – Hbg: 5. 5 g/d. L WBC: 21. 6 K; flow cytometry negative Urine culture: positive for E coli On 2/8/2014, DAT was positive for C 3 (2+) and negative for Ig. G On 2/9/2014, DAT remained positive for C 3, negative for Ig. G Antibody screen: non-specific reactions at room temperature but negative at 30 C – A cold agglutinin titer of <1 was found • 2 units p. RBC (both B Rh negative) were transfused, on 2/8 and 2/9/14 – Hbg appropriately increased (7. 0 Hbg) • A Donath-Landsteiner test was requested.
10 m. L patient serum Donor RBCs (group O) in all
10 m. L patient serum 5 m. L patient serum; 5 m. L fresh donor serum
10 m. L patient serum 5 m. L patient serum; 5 m. L fresh donor serum 10 m. L fresh donor serum Incubation 30’ @ 0 C 60’ @ 37 C 90’ @ 0 C 90’ @ 37 C Donath-Landsteiner Test • A 1 -A 2 show hemolysis, confirming presence of Donath-Landsteiner antibody • A 3 -C 3 must also be negative
Paroxysmal Cold Hemoglobinuria • An autoimmune hemolytic syndrome most often seen in children following infection by mumps, CMV, EBV, VZV, adenovirus, M. pneum, influenza, H. influenza, and E coli – Historically, PCH was also seen in syphilitic patients – Never occurs in older pts unless severe syphilis • Autoanti-P aka Donath-Landsteiner (DL) antibody – Ig. G, biphasic autohemolysin capable of binding to RBCs at cold temperatures and causing intravascular hemolysis of those cells at body temperature – Releases at high temp • Thermal amplitude rarely exceeds 20 C • Can present suddenly with severe hemolysis with an initial Hg of 7 g/d. L or lower • Labs: intravascular hemolysis, erythrophagocytosis on peripheral smear (highly suspicious for PCH)
Paroxysmal Cold Hemoglobinuria • Because the autoantibody in PCH rarely reacts above 4° C in vitro, routine Ab screens are usu negative, and crossmatches are compatible. • Patient RBCs sensitized by the DL antibody will most commonly give a positive DAT (DAG negative; DAC positive) – In addition, the DAT is positive only during or immediately after an episode of hemolysis – Because the antibody dissociates easily from RBCs during washing, the DAT is usually negative with anti-Ig. G. – Ig. G may be detected, however, if the cells are washed with cold saline and tested with cold anti-Ig. G reagent • Because the antibody is biphasic, many clinicians recommend keeping the patient warm and utilizing a blood warmer for transfusion. • Although PCH is due to an autoanti-P, it is not necessary to transfuse the patient with rare, P-negative red cells. • Self-limited, tx is steroids (unless caused by syphilis- killing bug stops PCH)
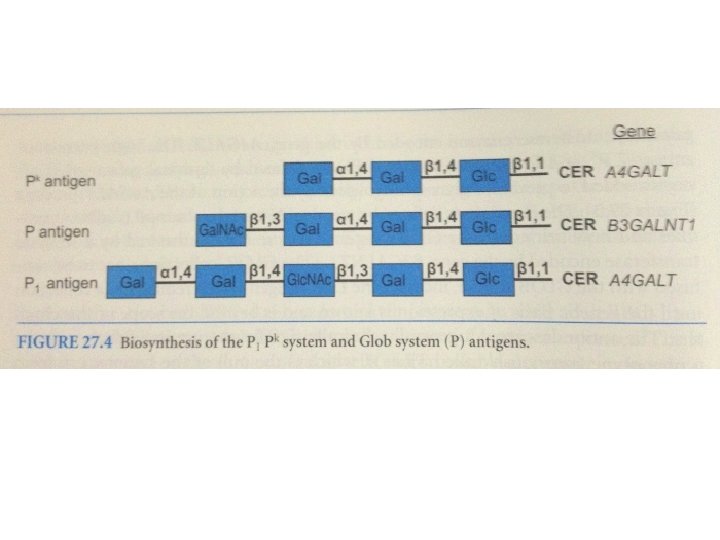
P 1 PK Blood Group System • Antigens: PK and P 1 (formerly P) • Defined by terminal galactosyl sugars on precursor glycosphingolipids or N-acetylgalactosyl (Gal. NAc) • PK: alpha-galactose on lactosylceramide – All RBCs express weakly • P 1: alpha-galactose on paragloboside – Receptor for microorganisms, E. coli and Streptococcus suis • P: – Receptor for parvovirus B 19 (erthema infectiosum)