Infant Childhood Adolescent Nutrition HLTH 120 N LECTURE



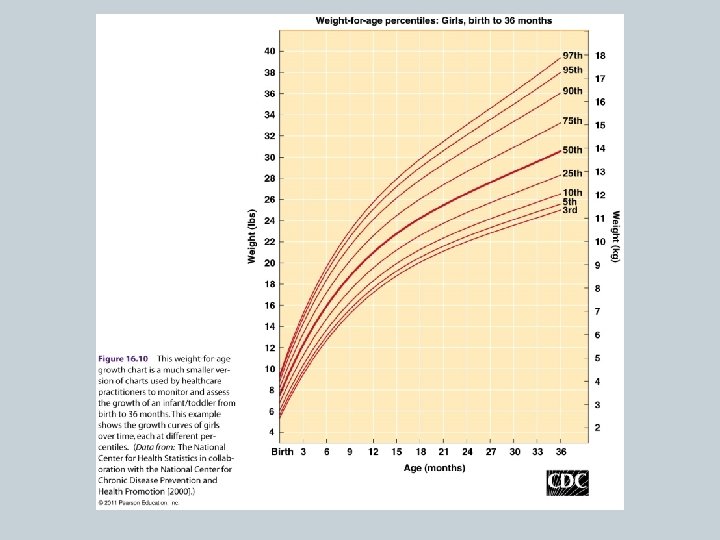






 Weight below the 3 rd percentile �Stunting")























- Slides: 38
Infant, Childhood & Adolescent Nutrition HLTH 120 N; LECTURE 17
Objectives �Relate nutrient needs to growth & activity patterns from birth through adolescence �Identify factors that impact allergy risk in infants & toddlers �Identify benefits & drawbacks of school breakfast & lunch �Recognize common deficiencies in adolescents as well as foods consumed in excess �Identify factors that impact risk of childhood and adult obesity
Infant Nutrition �First year of life 10” growth, triples in weight Very high BMR for weight �Organs and nervous system continue to develop and mature �Growth charts track growth main tools to assess nutritional status Limitations
Nutrient Needs for Infants Infant nutritional needs are unique: �High energy needs per unit body weight to support rapid growth - kcal/lb/day - % calories from fat Up to 20% calories from protein �Immature digestive tracts and kidneys �Small size
Nutrient Needs for Infants �High requirement: Iron, vitamin D, zinc, fluoride, B 12 �Vitamin injections �Fluids: at greater risk of dehydration ounces of fluid per pound of body weight Breast milk/formula: almost always adequate Avoid sweet beverages
Infant Formula �Formulas cannot duplicate immune factors, enzymes, and other unique components of human milk �Soy-based formulas: effective alternatives �Specialized formulas for specific medical conditions �Cow’s milk introduced:
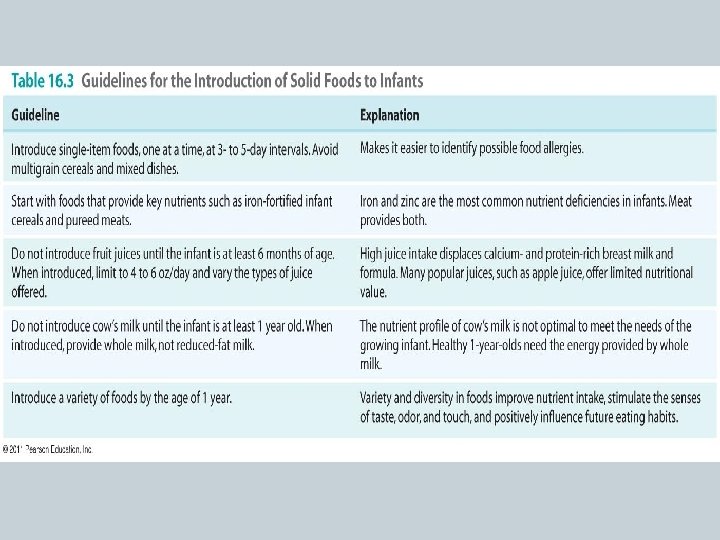
Starting Solid Foods �Declining nutrient stores & continued growth Complementary foods needed at months �Extrusion reflex lessens at 4 or 5 months �Must have muscular control of the head and neck �Sufficient maturity of the digestive tract & kidney
What Not to Feed an Infant � � �Corn syrup or honey �Sugary drinks �Excess salt and sugar �Too much breast milk or formula
Allergies �Most common foods: �Reduce the risk/ control exposure: Breastfeed Delay introducing solid foods until 6 months Introduce foods in isolation �Symptoms: GI distress, rashes, hives, runny nose, sneezing, difficulty breathing
Growth Problems � Failure to Thrive (FTT) Weight below the 3 rd percentile �Stunting low height-for-age � Acute and chronic malnutrition �Psychosocial factors: Poverty, poor knowledge, extreme nutritional beliefs, social isolation, domestic violence, and/or substance abuse
Dehydration Reflux �Extremely dangerous �“Spitting up” �Caused by �Common in preterm infants �Avoid overfeeding, keep �Physician may recommend pediatric electrolyte solution infant upright after feeding, watch for choking/ gagging
Baby Bottle Syndrome �Infants should never be left alone with a bottle; especially with high-carbohydrate fluids �Encourage using a cup by 8 months �Wean from bottle by 18 months
Lead Poisoning �Neurotoxin The brain and nervous system are still developing Decreased mental capacity & behavior, anemia, impaired growth �Allow tap water to run before use �Use only cold tap water for drinking, cooking, and infant formula preparation �Professionally remove lead-based paint
Toddlers � 12 to 36 months Rapid growth rate begins to slow Gain 5. 5 to 7. 5 inches, average 9 to 11 pounds Higher energy expended – why? Increased nutrient needs based on their larger body size � Needs will vary depending on exactly what age
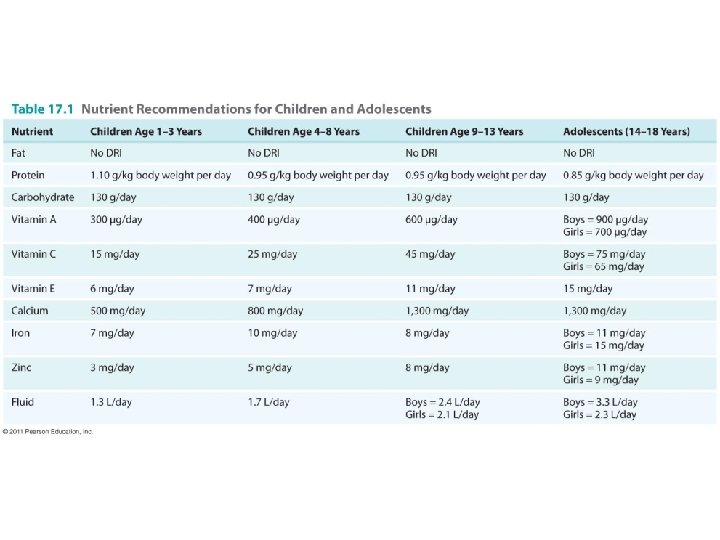
Toddlers �Macronutrients 30− 40% of total kcal from fat 1. 1 grams of protein per kg body weight 130 grams carbohydrates per day (most of the carbohydrates should be complex) grams fiber per 1, 000 kcal/day �Micronutrients Ensure adequate intake from fruits and vegetables � vitamins A, C, E, calcium, iron, zinc, potassium Drink whole milk until age �Supplements – when? .
Nutritious Food Choices & Allergies �Healthful variety of food available �Food should not be forced on a child �Frequent small meals for small stomach �Role modeling �Continue to watch for common food allergies:
Vegetarian Families �Vegan diet may be low in: �Too much fiber? may impair iron & zinc absorption May promote a premature sense of “fullness” �Fortified foods and supplements
Children �Growth slows again 2– 4 in. /year �Most nutrient needs increase �My. Pyramid for Kids �DRI values differ for boys & girls beginning at age 9
Macronutrients � 25− 35% of total energy from fat grams carbohydrate per day � 14 grams fiber per 1, 000 kcal grams protein per kg body weight � Micronutrients �Major Concern: �“Milk displacement” low-calcium diets also tend to be low in other nutrients �RDAs for iron and zinc also increase
What impacts choices? �Peers �Family �Media �School
School �School breakfasts Contribute to energy intake Avoid behavioral and learning problems �School lunches Government incentives vs. corporate incentives �Issues in schools
Adolescents �Adolescence continues to 18 years �Puberty: secondary sexual characteristics develop capacity for reproduction Emotions/behaviors unpredictable and confusing �Health Concerns
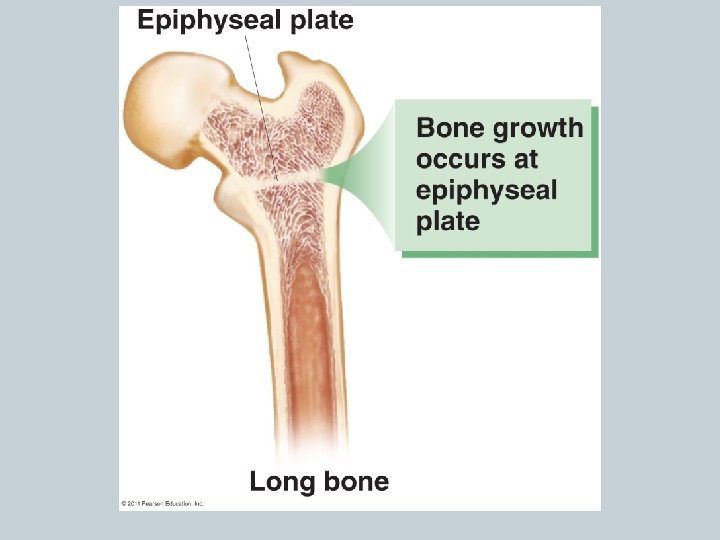
Adolescents �Growth spurts begin at age 10− 11 for girls, 12− 13 for boys �Average 20− 25% increase in height �Weight and body composition change �Skeletal growth
Macronutrients �Energy needs based on � gender, age, activity level, height, weight % of total energy from fat �<10% of total energy from saturated fat � % of kcal from carbohydrates � grams protein per kg body weight � 26− 38 grams of fiber per day
Micronutrients �Calcium intake Work to build up 1, 300 mg/day �Iron needs �Vitamin A role �Supplements Not a substitute for diet .
Fluid Needs �Proper hydration is essential especially with high activity �Boys: 11 cups/day �Girls: 10 cups/day �Water is best
Pediatric Obesity �Overweight: BMI above the 85 th percentile �Obese BMI above the 95 th percentile �Higher risk of health problems: Asthma Sleep apnea Impairs mobility Low self-esteem Social isolation
Pediatric Obesity �Increased health risks Gallstones Depression �Reversal Dieting that allows for continued development Physical activity Nationwide health campaigns?
Pediatric Obesity �Monitor if >80 th percentile for weight during toddler years �Encourage physical activity �Limit foods with low nutrient density �Early intervention most effective
Obesity Prevention - Family �Provide nutritious foods �Encourage a healthful breakfast �Sit down meals as much as possible Encourage attentive eating & enjoyment of food �Parents Retain control over purchasing & preparation
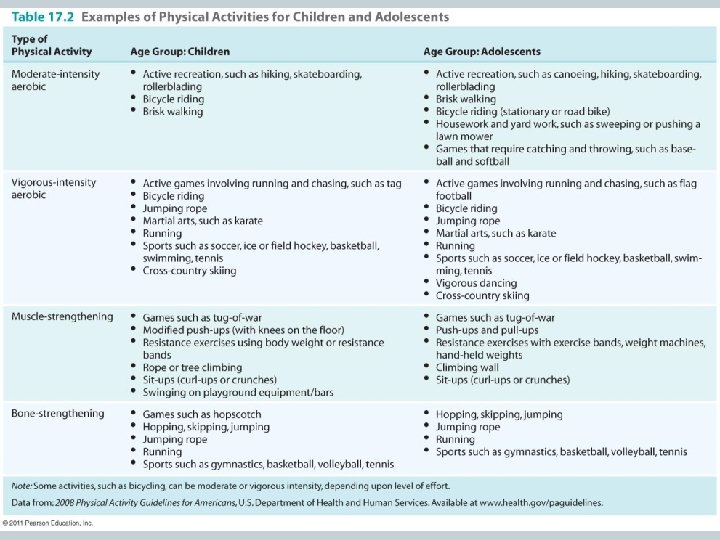
Physical Activity �Recommendation: Daily PA & exercise for at least each day �Bone- and muscle-strengthening activities �Non-competitive, fun, structured activities Allow self-pacing �Fitness Pyramid for Kids
Physical Activity �Role Models? �Shared activities �Television/electronic games Less than hours/day �Electronic games virtual tennis, step aerobics, dancing, other active simulations
Physical Activity �Physically fit children: Have improved behavior Are more attentive Are more focused Have higher levels of academic achievement �Activity needs to be promoted in schools! Parents, healthcare providers, and community members