Infant Mortality and Nutrition Primer ASTPHND MCH Nutrition

























- Slides: 26
Infant Mortality and Nutrition Primer ASTPHND, MCH Nutrition Council October 16, 2012 Jamie Stang, Ph. D, MPH, RD, LN University of Minnesota School of Public Health Associate Professor Director of Leadership Education and Training Program in Maternal and Child Health Nutrition, Co-Director Midwest Center for Lifelong Learning in Public Health
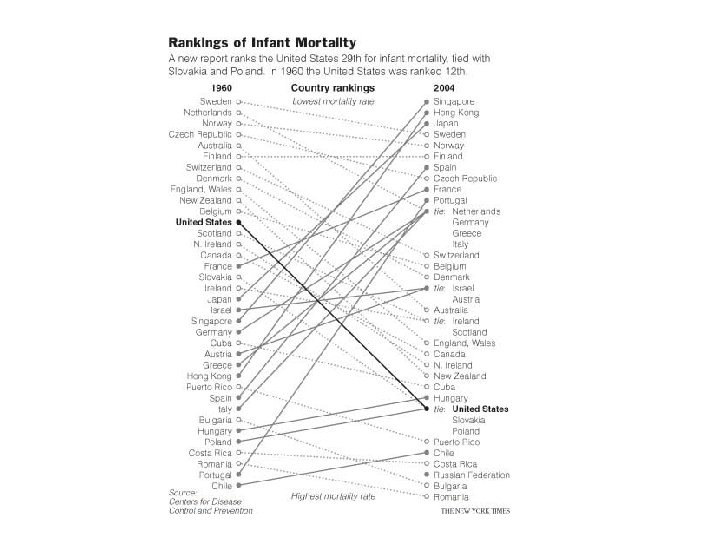
Infant Mortality • Infant mortality is defined as the probability of dying between birth and one year of age – Reported as rate per 1000 live births • US ranks 31 st in the world for infant mortality – Ranking of US has decreased in past decades • 2012 report by Congressional Research Service provides an overview of factors associated with infant mortality rates
Source: Adapted by CRS from Ariadi M. Minino, et al. , National Vital Statics Reports: Deaths: Final Data for 2008, National Center for Health Statistics, Vol. 59, No. 10, Hyattsville, MD, December 7, 2011.
Total and Preterm-Related Infant Mortality Rates
Leading Causes of Infant Mortality • Birth defects • Low birthweight including preterm birth and fetal growth restriction • Sudden Infant Death Syndrome • Maternal complications of pregnancy
Causes of Infant Mortality
Causes of Infant Mortality by Race
Infant and Fetal Mortality by Gestational Age
Nutrition’s Role in Infant Mortality “Every single cell, organ, and system inside a newborn baby comes mostly from her mother’s food intake before or during pregnancy. Maternal nutrition is a critical determinant of infant health; thus, it is not hard to see that poor maternal nutrition can contribute, directly or indirectly, to infant mortality. ”
Nutrition and Infant Mortality Good evidence for nutrition role in: • Birth defects • Preterm birth • Fetal growth restriction • Maternal complications of pregnancy such as preeclampsia, anemia, infections / inflammation
Nutrition’s Role in Infant Mortality Nutrition plays a key role in preventing several leading causes of infant mortality, but only as part of a long-term and integrated strategy for improving maternal and family health.
Birth Defects Folic acid status is associated with spina bifida, anencephaly, and other neural tube defects B vitamins, vitamin K, magnesium, copper, and zinc deficiencies have also been linked to other birth defects Vitamin A and other nutritional excesses can lead to congenital anomalies Poorly controlled diabetes, prior to and early in pregnancy, increases the risk cardiac and neural tube defects Dietary restrictions in women with PKU early in pregnancy have shown to reduce the risk of congenital malformations
Prevalence of Pre-pregnancy Obesity
Diabetes Second most frequently reported medical risk factor during pregnancy Pre-gestational Diabetes • Fetal death and congenital anomalies if poorly controlled • Poor control increases risk of cardiac defects Gestational Diabetes • Increased risk of fetal macrosomia, birth trauma, newborn hypoglycemia and hyperbilirubinemia. • May lead to insulin and leptin resistance in the fetus, and later greater susceptibility to diabetes and obesity
Low Birthweight and Preterm Birth • LBW and preterm birth are associated with prepregnancy weight status and weight gain during pregnancy • Most pregnant women in the U. S. enter pregnancy overweight or underweight • The majority of US women do not gain within the IOM recommendations • Maternal underweight and low weight gain during pregnancy are declining • Prepregnancy overweight/obesity and excessive weight gain during pregnancy are increasing
Weight, Weight Gain and Pregnancy • Low prepregnancy BMI and poor weight gain are associated with increased risk for – preterm birth – fetal growth restriction – important causes of infant mortality • The lower a woman’s BMI, the more likely she is to be undernourished. • Underweight prior to pregnancy increases the risk of congenital anomalies – Cleft lip and palate
Weight, Weight Gain and Pregnancy • High prepregnancy BMI and excessive weight gain are associated with increased risk of – – gestational diabetes preeclampsia postpartum hemorrhage fetal macrosomia and shoulder dystocia • Maternal obesity has been linked to increased risk of – neural tube defects and fetal death – indicated preterm delivery secondary to pregnancy complications • Excessive weight gain increases likelihood of excessive postpartum weight retention
Nutrition and Maternal Complications • Vitamin A, zinc and other micronutrients may influence maternal infection rates • Antioxidants may play a role in modulating inflammation • Fatty acid composition of diet may influence risk of preterm birth – Meta-analysis of studies of n-3 fatty acids showed decreased risk of preterm birth (RR 0. 61, CI 0. 40 -0. 93) • Gestational age was increased by 4. 5 days • Birthweight increased by 71 grams
Anemia • Maternal anemia contributes to maternal and fetal/infant morbidities and mortality associated with obstetrical hemorrhage • Deficiencies of iron, folate, and vitamin B 12 are main contributors to anemia – Other nutrients such as vitamins A, C and B 6 may also contribute to anemia • Strong evidence exists for an association between maternal hemoglobin concentration and both birthweight and preterm birth.
Other Associations • Periconceptional nutrition may be important the pathogenesis of preeclampsia – – Calcium Other minerals (copper, zinc) Anti-oxidants (vitamins C, E) n-3 fatty acids • Maternal nutrition can also mediate or modulate several of the major pathways (e. g. , inflammatory) leading to spontaneous preterm birth
Dietary Patterns Among Pregnant Women • Leading sources of energy from carbohydrates include: soft drinks, fruit juices, biscuits, muffins, white bread and other refined carbohydrates • Leading sources of energy from fats include: mayonnaise, salad dressings, whole milk, French fries and fried potatoes
Dietary Patterns Among Pregnant Women Consume more protein, fat and trans-fat, and carbohydrates than recommended. A substantial proportion of pregnant women do not meet their recommended daily intake for iodine, calcium, magnesium, iron, zinc, vitamins A, B 1, B 2, B 3, B 6, B 12, and vitamin C from food sources. Dietary intake of folate is inadequate for over 95 percent of women, and that of vitamin E is inadequate for 25 percent of pregnant women, which perhaps reflects low intakes of fruits and vegetables. 1 in 4 women does not consume adequate amounts of folic acid and vitamin E, even when multivitamins are included Fasting, pica, and fast food consumption are common among pregnant women
PHN Role in Infant Mortality Reduction Encouraging women to reach and maintain healthy body weight and waist circumference Supporting healthy eating patterns for women and families Encouraging appropriate weight gain during pregnancy Offering preconception care for women considering pregnancy healthy weight addressing chronic conditions and risk factors
PHN Role in Infant Mortality Reduction Supporting breastfeeding initiation and continuation Addressing hunger and food insecurity Monitoring and evaluating nutritional risk among women Engaging in program development, policy, systems and environmental change activities to support the health of women of reproductive age.
Suggested Readings Maternal Nutrition and Infant Mortality in the Context of Relationality by Michael C. Lu and Jessica S. Lu (2007) Joint Center for Political and Economic Studies The US Infant Mortality Rate: International Comparisons, Underlying Factors, and Federal Programs by Elayne J. Heisler (April 4, 2012) Congressional Research Service Mac. Dorman MF. Race and ethnic disparities in fetal mortality, preterm birth, and infant mortality in the United States: an overview. Smein Perinatol. 2011; 35: 200 -208 Slavig JD, Lamont RF. Evidence regarding and effect of marine n-3 fatty acids on preterm birth: a systematic review and meta-analysis. Acta Obst Gynec. 2011; 90: 825 -838