Using Mortality Risk Scores for Longterm Prognosis of






 0 -13分 0 -2分: 7. 1% 3 -6分: 19.")
 functional ability > 4 weight loss shortage of breath swallowing")






 yielded MMRI scores from 0 to 14")













- Slides: 32
Using Mortality Risk Scores for Long-term Prognosis of Nursing Home Residents: Caution Is Recommended Huang Liqun 2016 -08 -23
Magzine Journal of Gerontology:MEDICAL SCIENCE SCI/SCIE、SSCI Monthly series a: biological science/ medical science series b: psychological sciences and social sciences Appropriate areas include, but are not limited to, basic medical science, clinical epidemiology, clinical research, and health services research for professions such as medicine, dentistry, allied health sciences, and nursing.
Authors Robin L. Kruse Department of Family and Community Medicine, School of Medicine, University of Missouri-Columbia, Columbia
Background important 1. mid- and long-term prognosis difficult predict 2. statistical models 3. MMRI care planning mortality risk of dying in the subsequent 6 months logical focus 4. independent variables MDS This report focuses on comparing four predictive models that use MDS data to determine 6 -month mortality risk.
Background Flacker–Kiely model using MDS data for 780 residents who had been in a single facility for at least 1 year. Flacker--R model using MDS data from New. York state for residents who had been in the facility for at least 1 year. MMRI-R during the course of our study. This report focuses on comparing four predictive models that use MDS data to determine 6 -month mortality risk.
MMRI-R
Flacker model (1 -year mortality) 0 -13分 0 -2分: 7. 1% 3 -6分: 19. 2% 7 -10分: 50. 5% 11 -13分: 85. 7% functional ability > 4 weight loss shortage of breath Swallowing problem male sex BMI ≦ 22 Congestive heart failure age > 88
Flacker-R model(1 -year mortality) functional ability > 4 weight loss shortage of breath swallowing problem male sex BMI ≦ 22 congestive heart failure age > 88 diabetes feeding tube Poor appetite
Methods Participants using assessment data for all residents in one 92 -bed facility in Columbia, Missouri. Assessments all quarterly and full MDS assessments performed from May 7, 2007 through October 26, 2007. Follow-up vital status ( facility,s social woker ) death dates ( local newspapers, the social Security Death Index )
Methods statistical analysis SAS 9. 1 1. simple baseline frequencies for each resident 2. risk score as the sole dependent variable and 6 month mortality as the dependent variable logistic regression to compare model performance
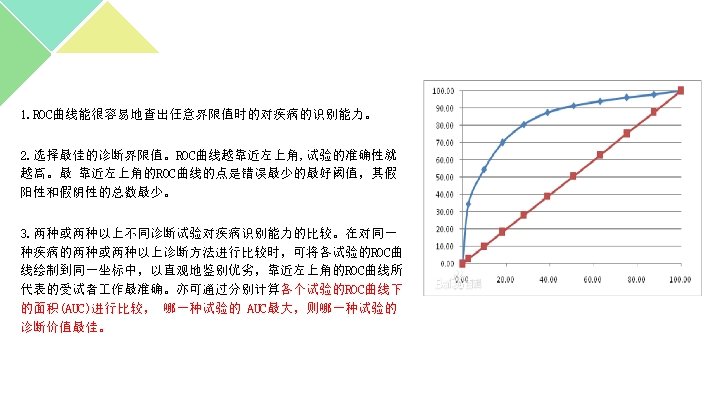
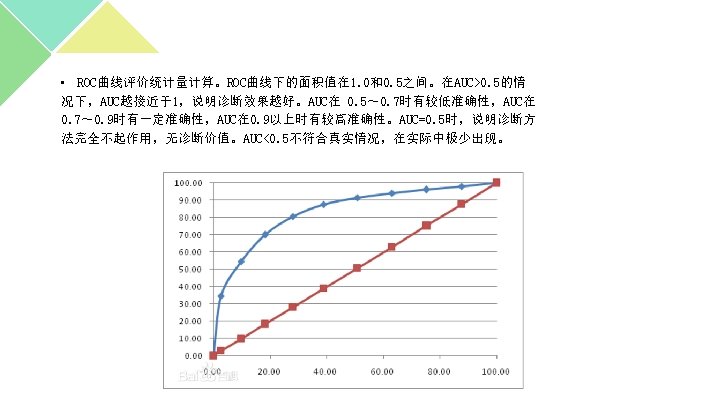
Methods statistical analysis 3. adjust for this “optimism” or overfitting a model to the peculiarities of a developmental data set heuristic shrinkage factor reduce the model parameter estimates intercept 4. c-statistic, to compare the models in terms of their discrimination, and indicates whether residents with higher mortality risk scores were more likely to die. 0. 5 -1. 0 indicates perfect discrimination 5. tested model calibration with the Hosmer-Lemeshow goodnesss-offit statistic
Methods statistical analysis 3. adjust for this “optimism” or overfitting a model to the peculiarities of a developmental data set heuristic shrinkage factor reduce the model parameter estimates intercept 4. c-statistic, to compare the models in terms of their discrimination, and indicates whether residents with higher mortality risk scores were more likely to die. 0. 5 -1. 0 indicates perfect discrimination 5. tested model calibration with the Hosmer-Lemeshow goodnesss-of-fit statistic
6. tested both Flacker models for their ability to predict 1 year mortality 7. 9 residents with unknown vital status at 6 months and 15 residents with unknown vital status at 1 year. excluding all individuals with unknown vital status assuming all were living 8. tested whether excluding short-stay residents, those discharged to home whithin 3 weeks of admission, would affect model performance.
Results 148 assessments for 130 residents. 114 residents had 1 assessment, 14 had 2, and 2 had 3. 27 of the 148 assessments within 6 -m were follow by mortality, 41 within 1 -y. 25 of 130 residents died within 6 -m, 38 within 1 -y.
Results The majority of assessments (125, 84%) yielded MMRI scores from 0 to 14 (0– 35 possible), putting the residents at less than 40% risk of 6 -month mortality. Only four residents had scores more than 18, indicating at least 60% mortality risk. 104 (70%) assessments scored less than 26 on the MMRI-R (0– 85 possible), with only four scores greater than 45 (>60% mortality risk). Scores were similarly restricted to the lower two thirds of possible scores for both Flacker models (0– 15 possible). 139 assessments, 3 -8. 20 residents, 7 -10. none were higher. Flacker-R model (0– 20 possible): 140 assessments, 3 to 10. 11 residents, 10– 11. the highest score in our sample was 12.
Results Imputing missing outcomes to “alive” had little effect on any of the models. Excluding 25 short-stay residents was associated with modest (0. 01– 0. 04) improvement in the c-statistic for the models.
Results Flacker model, one-year mortality Flacker-R model, one-year mortality MMRI model, six-month mortality Flacker-R model, six-month mortality MMRI-R model, six-month mortality
Results The heuristic shrinkage formula for the MMRI-R model was 0. 99. Thus, applying it to the model and refiting the intercept had almost no effect upon model discrimination or calibration in our data. Based on the large sample size, we would expect similar results for the MMRI. The sample used to develop the Flacker-R model was quite large, however, which would likely lead to a heuristic shrinkage factor near 1, as with the MMRI-R.
Discussion the models generally showed decreased discrimination relative to their initial development populations, with the c-statistic falling near 0. 7 or less for all models using our sample data. Flacker model for 1 -year: 0. 77 MMRI and MMRI-R: 0. 76 0. 69 0. 59 Flacker-R model for 1 -year mortality was 0. 71 in both its developmental population and our sample, suggesting good transportability.
Discussion The Hosmer–Lemeshow goodness-of-fit statistics for the Flacker and Flacker-R models were signifiant in the large data set that was used to develop the MMRI and MMRI-R models, indicating uneven performance across the range of predicted 6 month mortality.
Discussion Optimism can be assessed with either bootstrapping or the heuristic shrinkage factor, followed by shrinking model coeffiients. Due to the large size of the MMRI developmental sample, the factor was 0. 99; thus, adjustment had virtually no effect on model parameters.
Discussion In their original developmental populations, the MMRI and Flacker models showed equivalent discrimination. In our independent validation population, the c-statistics for these models were 0. 59 and 0. 69, respectively. Flacker-R model, showed somewhat lower discrimination in its developmental data set (0. 71), the c-statistic did not change in our sample data, suggesting that it transports well to external populations.
Discussion Resident characteristics can vary markedly between nursing homes, and staff in different facilities may employ slightly different coding practices, both of which can cause MDS data to systematically differ between facilities. It is diffiult to determine how these differences might affect the relationship between resident characteristics and mortality in an external population, particularly in a multivariable context. Despite these differences, both Flacker models performed reasonably well in our sample.
Discussion The models we tested were developed using full MDS assessments, although our sample included both full and quarterly assessments. we removed residents who were discharged within 3 weeks of admission from the models, but performance barely improved.
Discussion Few residents had mortality scores in the upper third of possible scores for any of the models. Predicted mortality for the highest risk stratum varied from 35% (MMRI 6 -month mortality) to 69% (Flacker-R 1 -year mortality). Both Flacker models, in particular the Flacker-R, do a better job at discerning which residents are at higher risk of mortality than either the MMRI or the MMRI -R. The Flacker-R has more variables. In contrast, the MMRI and MMRI-R fail to perform evenly across the spectrum of mortality risk. it overemphasizes complex relationships that are peculiar to its developmental data set.
Discussion We studied residents in one facility for several months, so our results may not generalize to residents of other nursing homes. a larger more representative sample Our sample of residents differed somewhat from the populations in which the models were derived. a longer period of data collection Mortality models could be added to the computerized MDS data entry system to provide risk scores in a timelier manner.
Both Flacker models had better discrimination and more reliably predicted high mortality risk than the MMRI models, making them better choices for identifying high-risk residents. With 6 -month mortality close to 20%, it could be reasonable to discuss palliative care planning for most residents who are anticipated to remain in the facility.
Thank you for you listening!