Estrogens 2 Metabolik Etkileri strojenler birok dokuyu etkiler

Estrogens 2

• Metabolik Etkileri. • • Östrojenler birçok dokuyu etkiler ve insanlarda ve hayvanlarda birçok metabolik etkiye sahiptir. Etkilerin doğrudan söz konusu doku üzerindeki hormon hareketlerinden veya ikincil olarak diğer bölgelerdeki eylemlerden kaynaklanıp kaynaklanmadığı her durumda net değildir. Kemik, vasküler endotel, karaciğer, CNS, bağışıklık sistemi, gastrointestinal (GI) yol ve kalp dahil olmak üzere çoğaltılamayan dokular, her iki östrojen reseptörünün düşük seviyelerini ifade eder ve ERa'nın ER to'ye oranı hücreye özgü bir şekilde değişir. Östrojenlerin birçok metabolik etkisi doğrudan etkilenen organlardaki reseptör aracılı olaylardan kaynaklanır. Östrojenlerin mineral, lipit, karbonhidrat ve protein metabolizmasının seçilmiş yönleri üzerindeki etkileri, farmakolojik etkilerini anlamak için özellikle önemlidir. • • • Metabolic Effects. Estrogens affect many tissues and have many metabolic actions in humans and animals. It is not clear in all cases if effects result directly from hormone actions on the tissue in question or secondarily from actions at other sites. Many nonreproductive tissues, including bone, vascular endothelium, liver, CNS, immune system, gastrointestinal (GI) tract, and heart, express low levels of both estrogen receptors, and the ratio of ERα to ERβ varies in a cell-specific manner. Many metabolic effects of estrogens result directly from receptor-mediated events in affected organs. The effects of estrogens on selected aspects of mineral, lipid, carbohydrate, and protein metabolism are particularly important for understanding their pharmacological actions.


• Östrojenlerin kemik kütlesi üzerinde olumlu etkileri vardır. • Kemik, osteoklastların rezorptif etkisi ve osteoblastların kemik oluşturucu etkisi ile kemik yeniden şekillendirme birimleri adı verilen bölgelerde sürekli olarak yeniden modellenir. • Toplam kemik kütlesinin korunması, erken yetişkinlikte (18 -40 yaş) olduğu gibi eşit oluşum ve emilim oranları gerektirir; bundan sonra emilim baskındır. Osteoklastlar ve osteoblastlar hem ERa'yı hem de ERβ'yi eksprese ederler, birincisi görünüşte daha büyük bir rol oynar. • Kemik ayrıca hem androjen hem de progesteron reseptörlerini eksprese eder. • Hayvan modellerine dayanarak, ERα'nın etkileri kemikte baskındır. • Östrojenler doğrudan osteoblastları düzenler ve tip I kollajen, osteokalsin, osteopontin, osteonektin, alkalin fosfataz ve diğer farklı osteoblast belirteçlerini sentezini arttırır. • Östrojenler ayrıca apoptozu inhibe ederek osteositin hayatta kalmasını arttırır. Estrogens have positive effects on bone mass (reviewed by Riggs et al. , 2002). Bone is continuously remodeled at sites called bone-remodeling units by the resorptive action of osteoclasts and the bone-forming action of osteoblasts. Maintenance of total bone mass requires equal rates of formation and resorption as occurs in early adulthood (ages 18 -40 years); thereafter resorption predominates. Osteoclasts and osteoblasts express both ERα and ERβ, with the former apparently playing a greater role. Bone also expresses both androgen and progesterone receptors. Based on animal models, the actions of ERα predominate in bone. Estrogens directly regulate osteoblasts and increase the synthesis of type I collagen, osteocalcin, osteopontin, osteonectin, alkaline phosphatase, and other markers of differentiated osteoblasts. Estrogens also increase osteocyte survival by inhibiting apoptosis.


Estrogens have many effects on lipid metabolism; of major interest are their effects on serum lipoprotein and triglyceride levels (Walsh et al. , 1994). estrogens slightly elevate serum triglycerides and slightly reduce total serum cholesterol levels. More important, they increase highdensity lipoprotein (HDL) levels and decrease the levels of low-density lipoprotein (LDL) and lipoprotein A (LPA) (Chapter 31). This beneficial alteration of the ratio of HDL to LDL is an attractive effect of estrogen therapy in postmenopausal women. • • • Östrojenlerin lipit metabolizması üzerinde birçok etkisi vardır; önemli olanlar serum lipoprotein ve trigliserit düzeyleri üzerindeki etkileridir. östrojenler serum trigliseritlerini hafifçe yükseltir ve toplam serum kolesterol seviyelerini hafifçe azaltır. Daha da önemlisi, yüksek yoğunluklu lipoprotein (HDL) seviyelerini arttırır ve düşük yoğunluklu lipoprotein (LDL) ve lipoprotein A (LPA) seviyelerini azaltırlar. HDL / LDL oranının bu yararlı değişimi postmenopozal kadınlarda östrojen tedavisinin çekici bir etkisidir.

Estrogen Receptors Estrogens exert their effects by interaction with receptors that are members of the superfamily of nuclear receptors. The two estrogen receptor genes are located on separate chromosomes: ESR 1 encodes ERα, and ESR 2 encodes ERβ. Both ERs are estrogen-dependent nuclear transcription factors that have different tissue distributions and transcriptional regulatory effects on a wide number of target genes (reviewed by Hanstein et al. , 2004). Ligands that discriminate between ERα and ERβ have been developed (Harrington et al. , 2003) but are not yet in clinical use. Both ERα and ERβ exist as multiple m. RNA isoforms due to differential promoter use and alternative splicing (reviewed by Kos et al. , 2001; Lewandowski et al. , 2002). The two human Ers are 44% identical in overall amino acid sequence and share the domain structure common to members of this family. • • Östrojen Reseptörleri Östrojenler etkilerini, nükleer reseptörlerin üst familyasının üyesi olan reseptörlerle etkileşime girerek uygularlar. İki östrojen reseptör geni ayrı kromozomlar üzerinde bulunur: ESR 1 ERa'yı ve ESR 2 ERİ'yi kodlar. Her iki ER de çok sayıda hedef gen üzerinde farklı doku dağılımlarına ve transkripsiyonel düzenleyici etkilere sahip östrojene bağlı nükleer transkripsiyon faktörleridir. • ERa ve ERβ arasında ayrım yapan ligandlar geliştirilmiştir. • Hem ERa hem de ERi, diferansiyel promotör kullanımı ve alternatif birleştirme nedeniyle çoklu m. RNA izoformları olarak bulunur. • İki insan Erisi, genel amino asit sekansında% 44 özdeştir ve bu ailenin üyeleri için ortak alan yapısını paylaşır.
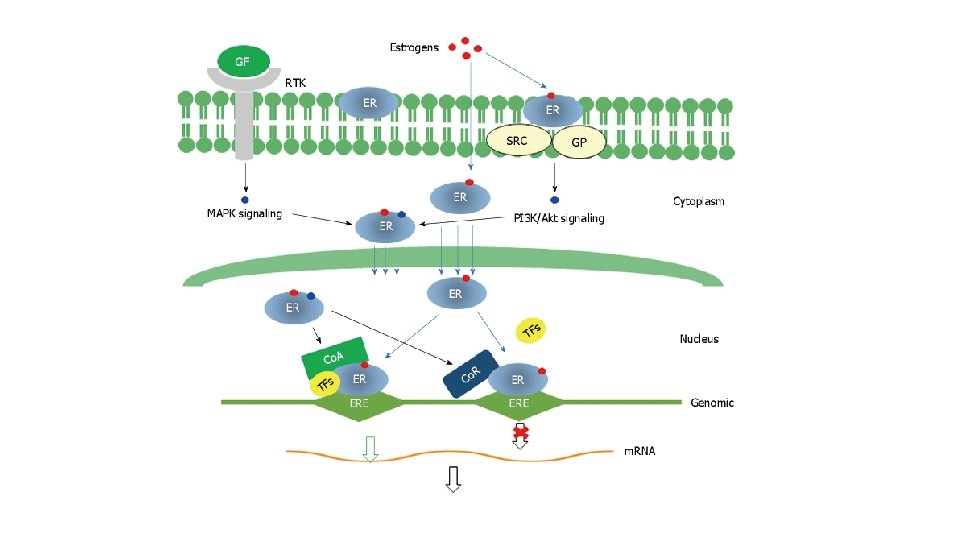
 are ligand-activated transcription factors that increase or")
Mechanism of Action Both estrogen receptors (ERs) are ligand-activated transcription factors that increase or decrease the transcription of target genes (Figure 40– 4). After entering the cell by passive diffusion through the plasma membrane, the hormone binds to an ER in the nucleus. In the nucleus, the ER is present as an inactive monomer bound to heat-shock protein 90 (HSP 90), and upon binding estrogen, a change in ER conformation dissociates the heat-shock proteins and causes receptor dimerization, which increases the affinity and the rate of receptor binding to DNA (Cheskis et al. , 1997). • Etki Mekanizması • Her iki östrojen reseptörü (ER), hedef genlerin transkripsiyonunu arttıran veya azaltan ligandla aktive edilen transkripsiyon faktörleridir. • Plazma zarından pasif difüzyonla hücreye girdikten sonra, hormon çekirdekteki bir ER'ye bağlanır. • Çekirdekte, ER, HSP 90 bağlı aktif olmayan bir monomer olarak bulunur ve östrojen bağlandığında, ER konformasyonundaki bir değişiklik, ısı şoku proteinlerini dağıtır ve afiniteyi artıran reseptör dimerizasyonuna neden olur. .

Absorption, Fate, and Elimination Various estrogens are available for oral, parenteral, transdermal, or topical administration. Given the lipophilic nature of estrogens, absorption generally is good with the appropriate preparation. Aqueous or oilbased esters of estradiol are available for intramuscular injection, ranging in frequency from every week to once per month. Conjugated estrogens are available for IV or IM administration. Transdermal patches that are changed once or twice weekly deliver estradiol continuously through the skin. Preparations are available for topical use in the vagina or for application to the skin. For many therapeutic uses, estrogen preparations are available in combination with a progestin. • • Emilim, Dagılım ve Eliminasyon Oral, parenteral, transdermal veya topikal uygulama için çeşitli östrojenler mevcuttur. • Östrojenlerin lipofilik yapısı göz önüne alındığında, emilim genellikle uygun preparasyonla iyidir. • Kas içi enjeksiyon için her hafta ila ayda bir sıklıkta değişen sulu veya yağ bazlı estradiol esterleri mevcuttur. • • • Konjuge östrojenler IV veya IM uygulaması için mevcuttur. • Birçok terapötik kullanım için, bir progestin ile kombinasyon halinde östrojen preparatları mevcuttur. Haftada bir veya iki kez değiştirilen transdermal patcler ciltte sürekli olarak estradiol salar. Vajinada topikal kullanım veya cilde uygulama için preparatlar mevcuttur.

Untoward Responses Estrogens are highly efficacious, but they do carry a number of risks. Many concerns arose initially from studies of early oral contraceptives, which contained high doses of estrogens. Oral contraceptives now contain much lower amounts of both estrogen and progestins, and this has significantly diminished the risks associated with their use. Nevertheless, major concerns about the use of estrogens remain today, especially regarding cancer, thromboembolic disease, and gallbladder disease. • Östrojenler oldukça etkilidir, ancak bir takım riskler taşırlar. • • Oral kontraseptifler artık hem daha düşük miktarlarda östrojen hem de progestin içerir ve bu, kullanımlarıyla ilişkili riskleri önemli ölçüde azaltmıştır. • Bununla birlikte, östrojen kullanımı ile ilgili, özellikle kanser, tromboembolik hastalık ve safra kesesi hastalığı ile ilgili önemli endişeler bugün devam etmektedir.
")
Therapeutic Uses The two major uses of estrogens are for menopausal hormone therapy (MHT) and as components of combination oral contraceptives (see final section of chapter), and the pharmacological considerations for their use and the specific drugs and doses used differ in these settings. Historically, conjugated estrogens have been the most common agents for postmenopausal use (0. 625 mg/day most often used). In contrast, most combination oral contraceptives in current use employ 20 - 35 μg/day of ethinyl estradiol. These preparations differ widely in their oral potencies (e. g. , a dose of 0. 625 mg of conjugated estrogens generally is considered equivalent to 5 -10 μg of ethinyl estradiol). Thus, the “effective” dose of estrogen used for MHT is less than that in oral contraceptives when one considers potency. Furthermore, in the last two decades the doses of estrogens employed in both settings have decreased substantially. The untoward effects of the 20 - to 35 -μg doses now commonly used thus have a lower incidence and severity than those reported in older studies (e. g. , with oral contraceptives that contained 50 -150 μg of ethinyl estradiol or mestranol) • • • Terapötik Kullanımlar Östrojenlerin iki ana kullanımı menopozal hormon tedavisi (MHT) içindir ve oral kontraseptif kombinasyonunun bileşenleri olarak ve bunların kullanım için farmakolojik düşünceler ve kullanılan spesifik ilaçlar ve dozlar bu ortamlarda farklılık gösterir. Tarihsel olarak, konjuge östrojenler postmenopozal kullanım için en yaygın ajanlar olmuştur (en sık kullanılan 0. 625 mg / gün). Buna karşılık, mevcut kullanımdaki çoğu oral kontraseptif, 20 -35 μg / gün etinil estradiol kullanır. Bu preparatlar oral alım güçlerinde büyük farklılıklar gösterir (örn. , 0. 625 mg konjuge östrojen dozu genellikle 5 -10 μg etinil estradiole eşdeğer kabul edilir).

Menopausal Hormone Therapy. The established benefits of estrogen therapy in postmenopausal women include amelioration of vasomotor symptoms and the prevention of bone fractures and urogenital atrophy. Menopozal Hormon Tedavisi. Postmenopozal kadınlarda östrojen tedavisinin yerleşik faydaları arasında vazomotor semptomların iyileştirilmesi ve kemik kırıklarının ve ürogenital atrofinin önlenmesi yer alır.

• • Menopausal Hormone Regimens. In the 1960 s and 1970 s, there was an increase in estrogenreplacement therapy, or ERT (i. e. , estrogens alone), in postmenopausal women, primarily to reduce vasomotor symptoms, vaginitis, and osteoporosis. • About 1980, epidemiological studies indicated that this treatment increased the incidence of endometrial carcinoma. • This led to the use of hormone-replacement therapy, or HRT, that includes a progestin to limit estrogen-related endometrial hyperplasia. Menopozal Hormon Rejimleri. 1960'larda ve 1970'lerde, menopoz sonrası kadınlarda östrojen replasman terapisinde veya ERT'de (yani sadece östrojenler), öncelikle vazomotor semptomları, vajinit ve osteoporozu azaltmak için bir artış oldu. 1980'lerde epidemiyolojik çalışmalar bu tedavinin endometriyal karsinom insidansını arttırdığını göstermiştir. Bu, östrojene bağlı endometriyal hiperplaziyi sınırlamak için bir progestin içeren hormon replasman tedavisi veya HRT kullanımına yol açtı.

• • • SELECTIVE ESTROGEN RECEPTOR MODULATORS AND ANTI-ESTROGENS In the past, estrogen pharmacology was based on a simple model of an agonist binding to a single ER that subsequently affected transcription by the same molecular mechanism in all target tissues and of antagonists that acted by simple competition with agonists for binding. This simple concept is no longer valid. By altering the conformation of the two different ERs and thereby changing interactions with co-activators and co-repressors in a cell-specific and promoterspecific contexts, ligands may have a broad spectrum of activities from purely anti-estrogenic in all tissues, to partially estrogenic in some tissues with antiestrogenic or no activities in others, to purely estrogenic activities in all tissues. The elucidation of these concepts has been a major breakthrough in estrogen pharmacology and should permit the rational design of drugs with very selective patterns of estrogenic activity. SEÇİCİ ESTROJEN RESEPTÖR MODÜLATÖRLERİ VE ANTİ-ESTROJENLER Geçmişte östrojen farmakolojisi, daha sonra tüm hedef dokulardaki transkripsiyonu ve basit rekabetle hareket eden antagonistleri tek bir ER'ye bağlayan basit bir agonist modeline dayanıyordu. bağlanma için agonistler. Bu basit konsept artık geçerli değil. İki farklı ER'nin konformasyonunu değiştirerek ve böylece hücreye özgü ve promotöre özgü bağlamlarda ko-aktivatörler ve ko-baskılayıcılarla etkileşimleri değiştirerek, ligandlar, tüm dokularda tamamen anti-östrojenik olandan, anti-östrojenik olan bazı dokularda kısmen östrojeniktir, bazılarında ise tamamen östrojenik aktivitelere karşı aktivitesi yoktur. Bu kavramların aydınlatılması östrojen farmakolojisinde önemli bir atılım olmuştur ve çok seçici östrojenik aktivite kalıplarına sahip ilaçların rasyonel tasarımına izin vermelidir.

• Selective Estrogen Receptor Modulators: Tamoxifen, Raloxifene, and Toremifene. • Selective estrogen receptor modulators, or SERMs, are compounds with tissue-selective actions. The pharmacological goal of these drugs is to produce beneficial estrogenic actions in certain tissues (e. g. , bone, brain, and liver) • Selektif Östrojen Reseptör Modülatörleri: Tamoksifen, Raloksifen ve Toremifen. Selektif östrojen reseptör modülatörleri veya SERM'ler, doku seçici etkilere sahip bileşiklerdir.
- Slides: 16