Care of Clients with Ear Nose and Throat


 – connects the cochlea, semicircular")


































- Slides: 40
Care of Clients with Ear, Nose and Throat Disorders Ian V. Sumagaysay, RN, MAN
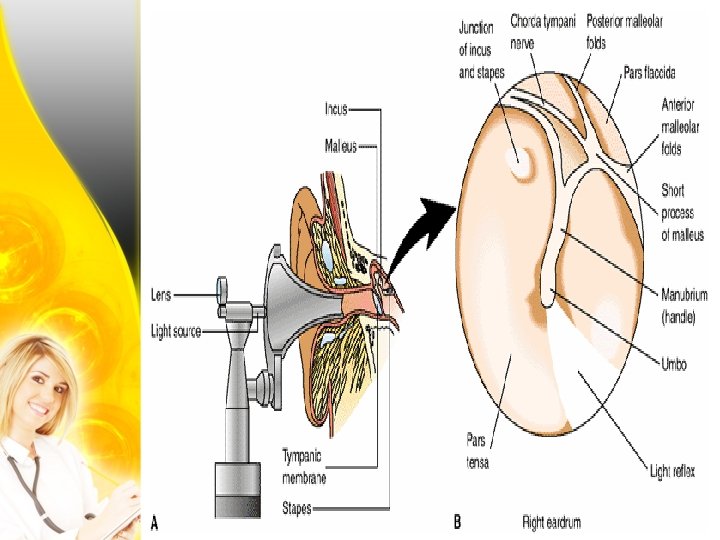
Structures of the Ear: 1. External Ears - auricle, external auditory canal and tympanic membrane/ ear drum. 2. Middle Ear – communicates with the mastoid air cells of the temporal bone. a. Ossicles (malleus, incus, stapes) – move and conduct sound waves from the external ear to the inner ear. b. Eustachian tube – connects the middle ear to the nasopharynx and equalizes pressure on both sides of the tympanic membrane. 3. Inner Ear ( Labyrinth) a. b. c. Vestibule – contains receptors that respond to the position of the head as it relates to gravity. Cochlea – organ of corti (receptor end organ of hearing) Semicircular Canals – sensory organs of equilibirum
Structures of the Ear: 4. Acoustic Nerve (CN VIII) – connects the cochlea, semicircular canals and vestibular receptors to the brain.
Structures of the Ear:
Structures of the Ear:
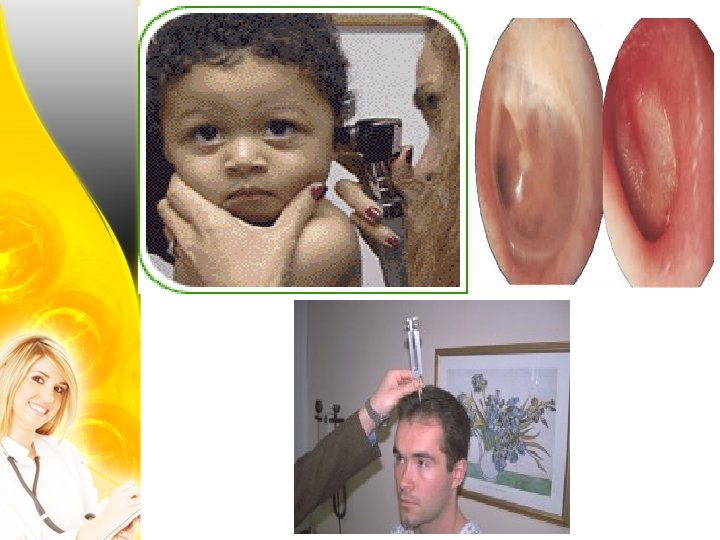
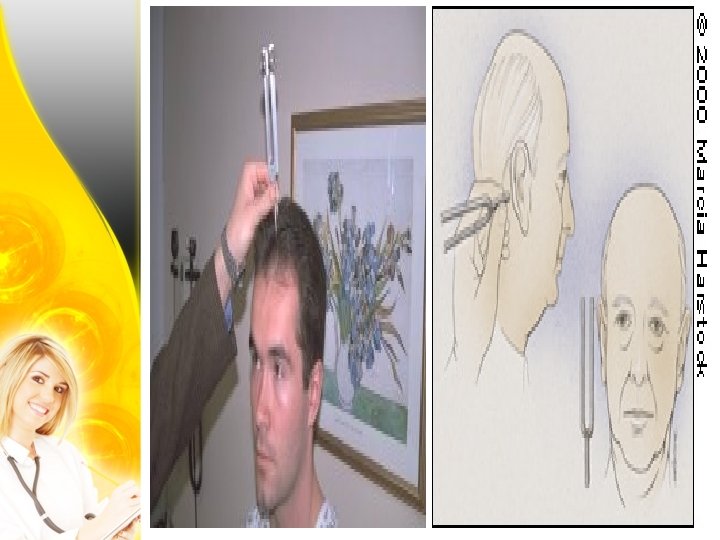
Functions: 1. Hearing 2. Positioning/ Balance Assessment: 1. HPI – trouble hearing, pain or discharges, tinnitus, complaints of dizziness or incoordination 2. Health history – age, heredity, allergies, upper respiratory infection, head trauma, excessive noise, ototoxic medications 3. Physical Assessment 4. Laboratory and Diagnostic Tests – otoscopic exam, hearing acuity screening, Weber’s Test (Bone Conduction), Rinne Test (Air Conduction), Audiometry (ASHA)
Nursing Dx: 1. 2. 3. 4. 5. 6. 7. Disturbed Auditory and Sensory Perception Risk for Injury Impaired verbal communication Acute pain Deficient knowledge Social isolation Anxiety
Nursing Management: 1. Promote measures that aid in maximizing the client’s auditory functioning 2. Prevent injuries 3. Enhance effective communication 4. Prevent or decrease pain and discomfort 5. Self care instructions 6. Prevent social isolation 7. Minimize anxiety 8. Prepare client for surgery 9. Take steps to prevent post op complications 10. Provide referrals
Conductive Hearing Loss Refers to various problems involving impaired passage of sound from the external ear and the inner ear caused by: - Impacted cerumen - External otitis media (fungal or bacterial) - Serous otitis media - Suppurative otitis media - otosclerosis – hereditary, women, aging 15 -30 years old
Conductive Hearing Loss Clinical Manifestations: - Cerumen impaction: visible - External otitis media: itching, pain, watery or purulent discharge - Serous otitis media: plugged feeling, reverberation of own voice, hearing loss - Suppurative otitis media: throbbing ear pain, fever, hearing loss, nausea and vomiting, pressure in the ear; red, bulging or retracted tympanic membrane - Otosclerosis: marked hearing loss, decreased air conduction on Rinne Test
Conductive Hearing Loss Treatment: - Soften cerumen with peroxide or glycerol - Ear irrigation for 2 -3 days - Otic solution for 15 mins. - Use of message board or hearing aid - Treat external otitis media with antibiotics and steriods - Myringotomy: incising the tympanic membrane to relieve pressure - Mastoidectomy: removal of the mastoid bone - Myringoplasty: repair of the tympanic membrane - Tympanoplasty: replacement of the middle ear structures - Stapedectomy: replacement of diseased ossicles with prostheses - Fenestration: creation of a new pathway for sound
Stapedectomy:
Meniere’s Disease A chronic disorder of the inner ear involving sensorineural hearing loss, severe vertigo, and tinnitus. - Cause is unknown; associated with aging, trauma or infection Assessment: - Sudden episodes of vertigo, unable to stand or walk, lasting for hours - Buzzing tinnitus - Nausea, vomiting and diaphoresis - Brief loss of consciousness
Meniere’s Disease Treatment: - Provide a safe, quiet enviroment - Bed rest - Antihistamines, antiemetics, mild diuretics - Low salt diet - Avoiding stimulants (smoking, caffeine, alcohol) - Anticholinergics, vasodilators - Labyrinthectomy: removal of the labyrinth or resection of the vestibular nerve - Endolymphatic decompression
Foreign Body Some objects are inserted intentionally into the ear by adults who may have been trying to clean the external canal or relieve itching or by children who introduce peas, beans, pebbles, toys, and beads. Insects may also enter the ear canal. In either case, the effects may range from no symptoms to profound pain and decreased hearing. Management: Removing a foreign body from the external auditory canal can be quite challenging. The three standard methods for removing foreign bodies are the same as those for removing cerumen: irrigation, suction, and instrumentation. The contraindications for irrigation are also the same. Foreign vegetable bodies and insects tend to swell; thus, irrigation is contraindicated.
Tympanic Membrane Perforation : Perforation of the tympanic membrane is usually caused by infection or trauma. Sources of trauma include skull fracture, explosive injury, or a severe blow to the ear. Less frequently, perforation is caused by foreign objects (eg, cotton-tipped applicators, bobby pins, keys) that have been pushed too far into the external auditory canal. Management: Although most tympanic membrane perforations heal spontaneously within weeks after rupture, some may take several months to heal. Some perforations persist because scar tissue grows over the edges of the perforation, preventing extension of the epithelial cells across the margins and final healing.
Hearing Aid A hearing aid is a device through which speech and environmental sounds are received by a microphone, converted to electrical signals, amplified, and reconverted to acoustic signals. Many aids available for sensorineural hearing loss depress the low frequencies, or tones, and enhance hearing for the high frequencies. Three types of implanted hearing devices are commercially available or in the investigational stage: the cochlear implant, the bone conduction device, and the semiimplantable hearing device.
Cochlear Implant Device
Bone Conduction Device
Semi-implantable Hearing Device
Structure and Function of the Nose, Throat and Sinus Nasal Passages or Turbinates – are three bony structures (superior, middle and inferior) located between the roof of the mouth and the frontal, ethmoid and sphenoid bones of the skull. Paranasal Sinuses (frontal, maxillary, ethmoidal and sphenoidal) – are cavities located around and draining into the nasal turbinates Phaynx (throat) – a tubelike structure connectibng the nasal and oral cavities to the larynx Larynx (voice organ) – is a cartilaginous epithelium lined structure connecting the pharynx and trachea
Structure and Function of the Nose, Throat and Sinus Epiglottis – a large valve flap of cartilage that covers the larynx during swallowing Glottis – opening between the vocal cords in the larynx Thyroid cartilage – lcargest cartilage in the trachea Cricoid cartilage – the only complete cartilaginous ring in the larynx below the thyroid cartilage Vocal cords – ligaments controlled by muscular movements to produce sound Palatine tonsils – located at either side of the uvula Adenoids (pharyngeal tonsils) – located at the roof of the nasopharynx
Structure and Function of the Nose, Throat and Sinus
Structure and Function of the Nose, Throat and Sinus
Structure and Function of the Nose, Throat and Sinus
Assessment 1. Health history – difficulty swallowing, cough, sore throat, fever, DOB 2. Allergies 3. Alcohol intake, smoking, URTI 4. PA, X-Ray Nursing Dx: 1. Ineffective breathing pattern 2. Risk for injury 3. Acute pain 4. Deficient knowledge 5. anxiety
Management 1. 2. 3. 4. Maintain patent airways Prevent injury Pain relief Minimize anxiety
Sinusitis An inflammation of the nasal sinuses that can be acute or chronic. Acute sinusitis is a result of an upper respiratory tract infection. Allergic or viral. Nursing management: 1. Nasal decongestant and antibiotics 2. Heated mist, warm compress and saline irrigations 3. Increase fluid intake 4. Avoid allergens
Pharyngitis An inflammation of the throat that can be acute or chronic. Acute pharyngitis is caused by a viral organism, Group A Streptococcus. Chronic pharyngitis is caused by dusty surroundings, excessive use of voice, chronic cough and habitual use of alcohol and tobacco. 1. Hypertrophic – generalized thickening 2. Atopic – late stage of hypertrophic; thin, whitish, glistening and wrinkled cartilage. 3. Chronic granular (cleryman’s sore throat) – marked by numerous edematous lymph follicles on the pharyngeal wall.
Pharyngitis Assessment: 1. Acute – fiery red pharyngeal membrane and tonsils, lymphoid follicles, enlarged and tender cervical lymph nodes, fever, malaise, sore throat 2. chronic – constant sense of irritation, fullness of throat, difficulty swallowing, mucus collection Management: 1. antibiotics, analgesics, antitussives, decongestants 2. Warm saline gargles, throat lozenges, ice collar, oral care 3. Soft or liquid diet, IOFI 4. Avoiding allergens and use of mask
Pharyngitis
Tonsillitis and Adenoiditis Inflammation of either the tonsils or adenoids. Caused by Group A Streptococcus infection. Signs and Symptoms: 1. Tonsillitis - Sore throat, fever, snoring, difficulty swallowing 2. Adenoiditis – mouth breathing, ear ache, draining ears, foul smelling breaths, noisy respirations Management: - Treat as pharyngitis, tonsillectomy, adenoidectomy
Tonsillitis and Adenoiditis
Epistaxis Severe nose bleeding. Caused by trauma, chemical irritation, infection, leukemia, blood dyscracias, HPN, medication Bleeding may occur through the nose, eyes or ears. Management: - Pressure over the nares for 10 -15 mins. - Nasal packing - Monitor bleeding
FBAO Occurs when there is a partial or complete occlusion of the larynx or lower airway by an aspirated object. Food is the most common cause of aspiration. Signs/sx: - Respiratory distress - Weak, ineffective cough, High pitched inspiration - Universal sign of chocking, Cyanosis, LOC Tx: - Heimlich maneuver, finger sweep, cricothyroidotomy
FBAO
FBAO