Anaphylaxis A Lifethreatening Emergency Anaphylaxis A serious allergic



 ¦ 21 – 49. 8 per 100,")















 ¦Same manifestations as at presentation recur up")















 and tissue (visceral) edema")



")



- Slides: 48
Anaphylaxis A Life-threatening Emergency 朱士傑 風濕免疫過敏科
Anaphylaxis ¢ A serious allergic reaction that is rapid in onset and may cause death
Anaphylactoid Reaction ¢ Ig. E-independent ¢ Clincially indistingushable from anaphylaxis ¢ 不建議使用
Anaphylaxis ¢ Incidence ¦ increasing (youngest, food) ¦ 21 – 49. 8 per 100, 000 personyears ( person-years) ¦Under diagnosis, under-reporting, a variety of definition
Anaphylaxis Is Not Rare Insect sting 3% of adults 1 -3% of children Food 1% of adults Drug 0. 1% of cases RCM 3% of patients Immuno Tx 1% of adults Latex 5% of adults
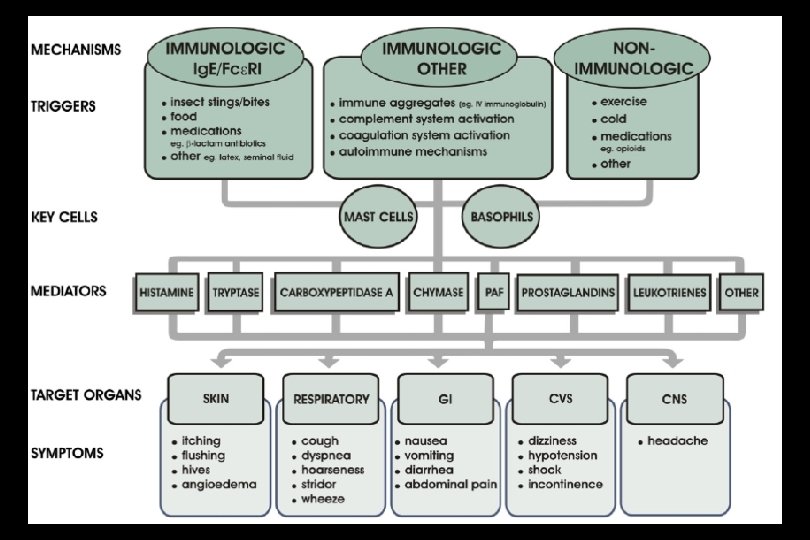
Mechanisms of Anaphylaxis n Type I hypersensitivity reaction n Allergen exposure n Production of allergen-specific Ig. E n Ig. E-sensitized mast cells and basophils n Ig. E-mediated degranulation upon reexposure to allergen
Mechanisms of Anaphylaxis n Complement activation ¦ Type II hypersensitivity ¦ Type III hypersensitivity ¦ Aggregated Ig Direct mast cell activation Drugs (e. g. ASA, vancomycin), exercise, cold, idiopathic n Ig. G-dependent (not proven in human) n
The activators of mast cells
Anaphylaxis Mediators n Histamine ¦ ¦ ¦ n H 1: smooth muscle contraction vascular permeability, vasodilatation H 2: vascular permeability H 1+H 2: vasoilatation, pruritus Leukotrienes ¦ ¦ Smooth muscle contraction vascular permeability and dilatation
Causes of Ig. E-Mediated Anaphylaxis n Antibiotics and other medications ¦ n Beta lactams, tetracyclines, sulfas, aspirin, ibuprofen Foreign proteins Latex, hymenoptera venoms, heterologous sera, protamine, seminal plasma, chymopapain allergen vaccines, polysaccharide ¦ n Foods ¦ n n Peanut, tree nuts, shellfish, milk, egg Exercise (possibly, in food- and medicationdependent events) Biologic agent: cetuximab, infliximab, omalizumab
Causes of Ig. E-independent Mediator Release n ¦ Complement activation-activation of contact system ¦ Radiocontrast media ¦ protamine (possibly) ¦ Dialysis membrane ¦ Ethylene oxide gas on dialysis tubing Direct release of mediators from mast cells and basophils ¦ Opiods ¦ Muscle relaxants ¦ Exercise ¦ Physical factors (heat, cold)
Causes of Ig. E-independent Mediator Release n n n Disturbance in arachidnoic acid metabolism ¦ Aspirin ¦ Nonsteroidal antiinflammatory drugs Immune aggregates ¦ Gammaglobulin ¦ Ig. G-anti-Ig. A ¦ Possible dextran and albumin Cytotoxic ¦ Transfusion reactions to cellular elements (Ig. G, Ig. M)
Incidence and/or Severity of Anaphylaxis Risk Factor n Age n Gender n Route of administration n Constancy of antigen administration n Time elapsed since last reaction n Atopy
Anaphylaxis - Clinical Manifestations n n n Cardiovascular ¦ Tachycardia then hypotension ¦ Shock: ≧ 50% intravascular volume loss ¦ Bradycardia (4%) (transient or persistent) ¦ Myocardial ischemia Lower respiratory - bronchoconstriction wheeze, cough, shortness of breath Upper respiratory ¦ Laryngeal/pharyngeal edema ¦ Rhinitis symptoms
Anaphylaxis - Clinical Manifestations n n Cutaneous ¦ Pruritus, urticaria, angioedema, flushing Gastrointestinal ¦ Nausea, emesis, cramps, diarrhea Ocular ¦ Pruritus, tearing, redness Genitourinary ¦ Urinary urgency, uterine cramps
Case 1 Woman aged 20, six months pregnant Trigger: Chinese meal Symptoms and treatment: one hour after start of meal felt faint; mild asthma; sever dyspnoea and laryngeal oedema; loss of consciousness; taken to emergency department after 10 minutes; on arrival cyanosed, respiratory arrest; periorbital oedema; salbutamol infusion; cardiac arrest four minutes later; adrenaline given; intubated with difficulty and ventilated Recovered Cause: allergy to green pepper
Case 2 Woman aged 30 Trigger: one teasponful muesli Symptoms and treatment: immediate itching of mouth; throat swollen and uncomfortable inside; vomited; dyspnea (could not breathe, different from her asthma); laryngeal edema (obstruction in throat); lightheaded; no loss of consciousness; used her own salbutamol inhaler (no effect); taken to emergency department; respiratory distress; intense erythema and generalised urticaria; given intramuscular adrenaline and chlorpheniramine Rapid recovery Cause: allergy to brazil nuts and hazelnuts
Case 3 Boy aged 8 months Trigger: Tiny quantity of peanut butter Symptoms: blisters around mouth; distressed; vomiting; dyspnea; urticaria Cause: allergy to peanuts Case 4 Woman aged 26 Trigger: vaginal examinations during labour Symptoms: itching of vulva; oedema of labia; generalised urticaria and pruritus; mild dyspnoea; felt woozy, lightheaded, odd, shaking Cause: allergy to latex rubber
Anaphylaxis -Temporal Pattern n Uniphasic Biphasic (3%-20%) ¦Same manifestations as at presentation recur up to 8 hours later Protracted ¦Up to 32 hours ¦May not be prevented by glucocorticoids
Food-Related Anaphylaxis n. Frequency: ~ 150 deaths / year n The most common single cause of anaphylaxis in ED in USA. (young) n. Risk: Underlying asthma Delayed epinephrine Symptom denial Previous severe reaction n. History: known allergic food n. Key foods: peanut/ nuts / shellfish n. Biphasic reaction n. Lack of cutaneous symptoms n. Schools, no predictive markers n. Exercise
Natural History in Food allergy n n n Dependent on food & immunopathogenesis ~ 85% Cow Milk, egg, wheat, soy allergy remit by 3 yrs ¦ Declining/low levels of specific-Ig. E predictive ¦ Ig. E binding to conformational epitopes predictive Allergy to peanut, nuts, seafood typically persisited
Peanut Allergy n Factors Associated with development of peanut allergy in childhood ¦ family history of peanut allergy ¦ occurrence of oozing crusted skin rashes, ¦ topical use of peanut-oil based preparation ¦ exposure to soy protein n Prevention ¦ Recombinant anti-Ig. E antibody ¦ Gene (naked DNA) immunization N E Engl J Med, march 13, 2003
Classification of Insect Sting Reactions n Normal Immediate, local, transient n Large local Delayed, prolonged, progressive n Systemic Immediate, generalized n Other Toxic, serum sickness
Natural History of Insect Sting Allergy n n Spontaneous loss of clinical venom sensitivity Adults differ from children Most fatal reaction on the first sting reaction Evolution of systemic reactions ¦ ¦ ¦ frequency and severity large local into systemic no predictive markers
Insect sting and bites Anaphylaxis Indications for Venom Immunotherapy 98% efficacy n Medical criteria ¦ ¦ n history of systemic reaction positive venom skin test Non-medical considerations ¦ ¦ age of patient alterations in life style co-existing diseases costs
Allergen Immunotherapy - Systemic Reactions n n n 10 -15% during initial immunotherapy, 1 -3% during maintenance Most in < 20 minutes, but severity worse with later onset Systemic reactions not preceded or predicted by large local reactions Not correlated with asthma in all studies Related to: dose/vial errors, unstable asthma, seasonal flare, extreme sensitivity, ß blockers, new vial / new extract, rush schedule Fatal reactions: 58 observed over 25 years: ¦ ¦ ¦ 90% in < 30 minutes 50% delayed use of epinephrine 25% prior systemic reactions – 30% due to errors – 50% with acute asthma – 25% peak pollen season
Anaphylaxis Exercise-Induced Syndrome n n n Prodrome - flushing, pruritus, fatigue Early - urticaria, angioedema Established - stridor, GI symptoms, collapse Late - headache Precipitating Events: isometric and isotonic exercise; hot environment, foods, medications Temporally unpredictable
Anaphylaxis Exercise-Induced Syndrome Treatment / Prevention Avoidance of exercise, especially in heat n Avoidance of allergenic foods before exercise n Buddy system-epinephrine n
Latex Allergy
Risk Groups for Latex Allergy n Patients with history of multiple surgeries ¦ Meningomyelocele or severe urologic anomalies n n Health care workers Other occupational exposure ¦ Rubber product workers, hair dressers, house cleaners n Individuals with atopy n n Hay fever, rhinitis, asthma, or eczema Patients with specific food allergies ¦ Banana, kiwi, avocado, chestnut, etc. ¦ Similar proteins
Latex Allergy n n n Most important step is avoidance of exposure in susceptible patients With universal precautions, the problem will likely worsen Hospitals should strive for low allergen environments ¦ Powderless gloves with low extractable protein content n Protect yourself ¦ Treat dermatitis ¦ Cover hand wounds with tegaderm
Anaphylactoid reaction to RCM n n IV, hysterosalpingogram, myelogram, retrograde pyelogram Frequence: 5 -8 %, 0. 1% for life-threating reaction 16% to 44% for repeated reaction Pretreatment and use of lower osomolar RCM, the risk is reduced to 1%
Drug Hypersensitivity Prevention Ascertain host risks n Avoid cross-reactive drugs n Use of predictive skin tests n Prudent use of drugs n Preferential use of oral drugs n
Anaphylaxis Fatalities ≈ 4% n Increased Risk ¦beta blockade, ACE inhibitors, severe hypotension, bradycardia, sustained bronchospasm, poor response to epinephrine ¦Adrenal Insufficiency ¦Asthma ¦Coronary Artery Disease n
Anaphylaxis Fatalities Post Mortem Findings n n n Airway (laryngeal) and tissue (visceral) edema Pulmonary hyperinflation Tissue eosinophilia Elevated serum tryptase Myocardial injury
Anaphylaxis Diagnosis Clinical Features n Histamine n Serum Tryptase measurable up to 6 hours n
Prevention of Anaphylaxis n History: drug, venom, food, latex reactions ¦ n n n Avoidance, Medic-Alert and ID card Penicillin skin tests & desensitization Administer drugs orally rather than parenterally when possible Hymenoptera avoidance & immunotherapy Iodinated Dye Pretreatment Avoid ¦ ¦ ¦ ß blockade in those on immunotherapy or at risk of Hymenoptera anaphylaxis Immunotherapy in those on ß blockers ACE inhibitors in food / Hymenoptera anaphylaxis
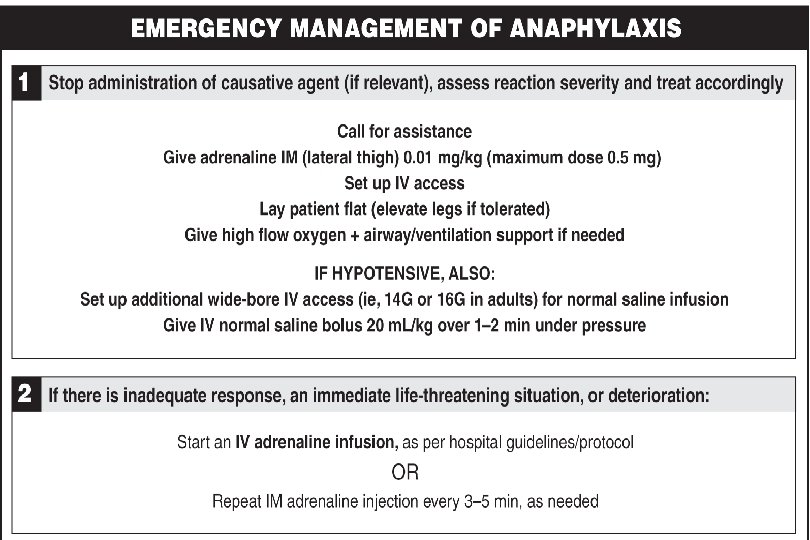
Management n n ABC’s, early airway intervention as needed Early administration of epinephrine n 0. 01 mg/kg - 0. 3 - 0. 5 mg, IM. Maximum dose, 0. 5 mg. n IV – 5 -10 μg (0. 2 μg/kg) for hypotension) 0. 1 - 0. 5 mg in cardiovascular collapse Remove allergen (stingers), or apply tourniquet if exposure site on extremity 2 large bore IV lines : n Volume resuscitate with crystalloid or colloid solutions
Management continued n n Glucagon 1 -5 mg IV (if epinephrine contraindicated or ineffective) (activate adenylate cyclase) Anti-histamines: ¦ ¦ n n n Benadryl 50 mg iv Pepcid 20 mg iv; Ranitidine 50 mg iv Corticosteroids (Hydrocortisone, prednisone, Methylprednisolone) Vasopressors: dopamine, levarterenol, vasopressin Ongoing evaluation of airway / vital signs
Anaphylaxis Treatment n Corticosteroids ¦ Not effective in protracted anaphylaxis ¦ Effective in iodinated dye prophylaxis ¦ The efficacy in anaphylaxis not established n Prolonged resuscitation
Risk Management for Anaphylaxis n Ask the questions n Prescribe epinephrine injector n Refer to allergy specialist
Epi. Pen® auto-injector