2009 Standardized Mortality Ratio Project Summary Svetlana Lana
 Kacherova, QI Director Lisle Mukai, QI")















 when planning")





 and it will")






 Kacherova, QI Director skacherova@nw 18. esrd. net Lisle Mukai, QI Coordinator lmukai@nw")
- Slides: 33
2009 Standardized Mortality Ratio Project: Summary Svetlana (Lana) Kacherova, QI Director Lisle Mukai, QI Coordinator ESRD Network 18 July 21, 2009
SMR Project: Inclusion Criteria for Participating Facilities SMR rated “Worse than expected” (2008 DFR data) – 26 facilities State Surveyors review DFRs before visiting facilities SMR information is available on the Dialysis Facility Compare website at www. medicare. gov 2009 DFRs just received: expect to receive your reports in August 2009 2
Project Timelines: Oct. 2009 – facilities notified Nov. 2009 – Web. Ex session Nov. - Dec. – Collection of the MD letters, Facility Process Checklists, RCA, and action plans (PDSA) Jan. – May 2009 – project implementation Feb. – March 2009 – Network follow-up (supportive documentation)
Network Role During the Project: Project Leader Supplied the templates for RCA & PDSA Supplied facilities with tools and knowledge Periodically monitored and provided feedback Conducted phone interviews to obtain facility-specific data Chased you for data & documentation Assisted your facility to stay in compliance with the QAPI program requirements 4
V 626 QAPI Condition Statement The dialysis facility must develop, implement, maintain and evaluate an effective, data driven, quality assessment and performance improvement program with participation by the professional members of the interdisciplinary team. . . …The dialysis facility must maintain and demonstrate evidence of its quality improvement and performance improvement program for review by CMS 5
Project Summary
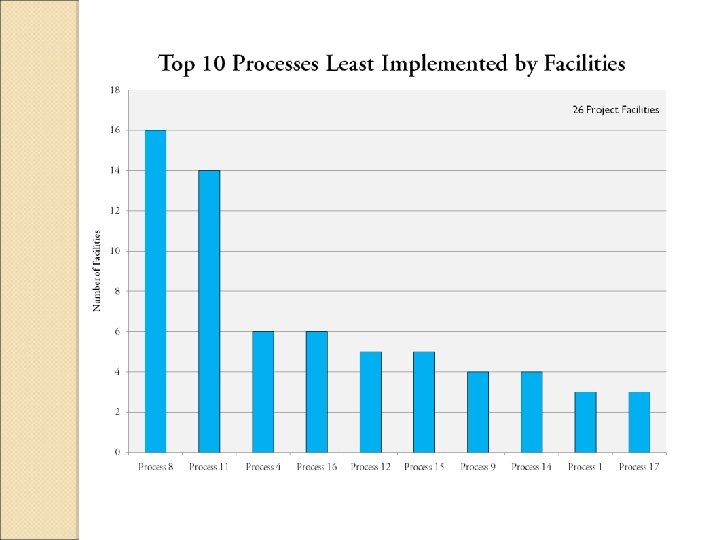
Top 10 Processes identified by facilities 1. Process #8: At least 85% of patients in the facility have hemoglobin above 11 gm/dl • The current standard for this indicator is Hgb between 10 -12 gm/dl. • For 2009 -2010 year, the Network goal for anemia will be: Ø 52% of patients on ESA therapy having a Hgb between 10 -12 gm/dl. Ø No more than 4% of patients with a Hgb <10 gm/dl
2. Process # 11: Less than 10% of patients in the facility have a catheter as a permanent vascular access. • Network & CMS goal is <10% of patients having a catheter greater than 90 days 3. Process # 4: Physicians participate in patient care meetings on a regular basis, ensuring that all patients are reviewed at least quarterly. • New Conditions for Coverage (494. 90)
4. Process #16: Facility staff accurately indicates cause of death when completing 2746 Death Notification forms for deceased patients. 5. Process # 12: At least 50% of patients in the facility have an AVF as permanent vascular access. • NW prevalent AVF goal for 2009 -2010 = 57. 8%
6. Process # 15: Facility staff reports all comorbidities when completing 2728 CMS Medical Evidence Forms for new ESRD patients. 7. Process # 9: At least 88% of patients in the facility have URR > 0. 65 (65%) or Kt/V > 1. 2. • This is the Network goal for the 20082009 year • PD goal = 88% of patients with Kt/V > 1. 7
8. Process # 14: Facility Nurse Manager has sufficient time to complete all administrative tasks and requirements (e. g. Network forms). 9. Process # 1: Physicians see patients and review records/orders at least weekly (new & unstable patients) and at least monthly (stable or long-term patients).
10. Process #17: Facility has a formal vascular access monitoring/intervention program. Per the Interpretive Guidelines: • “Monitoring” strategies include physical examination of the vascular access. • “Surveillance” strategies include devicebased methods.
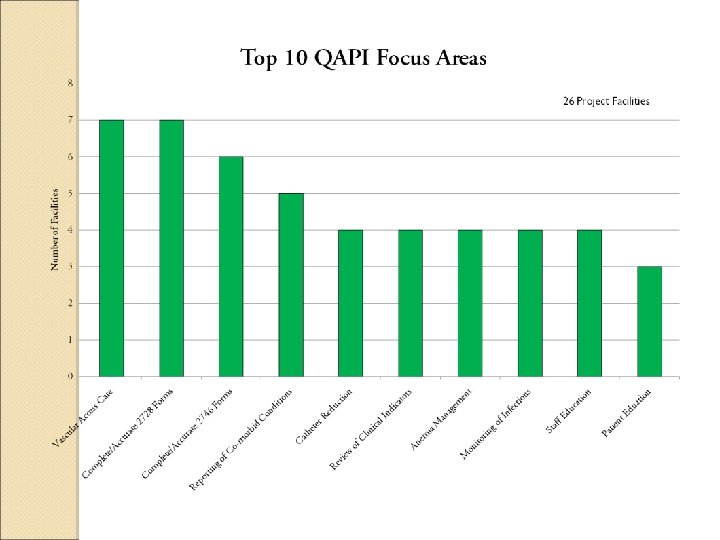
Summary of Strategies for the top 10 focus areas: Vascular Access Care: • Review of vascular accesses to ensure that the correct vascular access is recorded in the patient’s electronic records and facility tracking logs. • Staff education on vascular access care • Patient & family education on vascular access care
• • • Develop communication with physician regarding access placement prior to hospital discharge. Engage nephrologists & surgeons into the Fistula First program Find a good vascular access surgeon Use the Vascular Access Centers for vessel mapping, follow-up, and interventions. Develop & implement a catheter reduction program – addressing both prevalent & incident patients.
Complete/Accurate 2728 Forms: • Have the physician or the Clinical Manager review forms prior to submitting form to the Network
Complete/Accurate 2746 Forms: • Have the physician or Clinical Manager review forms prior to submitting form to the Network • AA will keep a binder of all 2746 forms and keep a log for all causes of death • Develop & implement a mortality tracking report
Reporting of Co-morbidities: • Review of medical records for co-morbid conditions (H&P) when planning care • Have physician review all co-morbid conditions prior to signing 2728 forms • Have physician include co-morbid conditions on the patient’s progress notes
Catheter Reduction: • Implementation of a catheter reduction program – addressing prevalent & incident patients • Nephrologist develop a relationship with surgeons and explain the importance of vascular access care with emphasis on AVFs
Review of Clinical Indicators: • Review of monthly lab results by the interdisciplinary team • Trend facility data for each indicator – assess need for improvement • Monitor outcomes by physician group and have the Medical Director maintain communication with the group regarding their statistics • Distribute physician or physician group QA reports of those patients that fall below the goal(s)
Anemia Management: • Identify patients with Hgb < 10 and develop Plan of Care • Protocol changes to reflect the new Conditions for Coverage • Designate hours for the Anemia Manager to perform duties
Monitoring of Infections: • Decrease catheter rate - Educating patients & families about benefits/disadvantages of catheters • Develop & implement an infection control log to track the types of infection, actions/interventions taken, date of resolution, and trending of types of infection and frequency of events • Monitor staff adherence to infection control policies • Encourage and remind patients to wash access prior to treatment
Staff Education: • Hold in-services Patient Education: • Staff to educate patients on compliance with dialysis prescription, diet, and vascular access care – focused education for specific issues • Social worker to check/assess all diabetic patients to see if they need more diabetes education and refer them to a diabetic center
Patients will be given a report card (phosphorus, potassium, etc. ) and it will be discussed with the dietitian on a monthly basis • Dietitian maintains communication with the family and/or nursing home regarding the patient’s diet • Lobby poster displays regarding patient issues the facility would like to address (i. e. fluid restricitons) •
• Facility host a nutritional day – Example: “Cheese Alternative Tasting Day” to provide a sampling of ricebased and soy-based cheeses in a variety of flavors to educate patients on cheese alternatives available
Other Focus Areas and Strategies Hospitalization: • Develop hospitalization tracking log – track suspected/actual causes for admission • Medical Director/Nephrologist to follow -up on all patients hospitalized > 4 days • Review of newly admitted unstable patients weekly with focused discussion on the patient’s needs
Review of patient assessment & Plan of Care monthly on all unstable patients • Review hospital admission & discharge reports to establish correct causes of admission, procedures performed, and medication changes • Patient education regarding good hygiene and prevention of illness •
Vaccination: • Designate a specific individual to oversee the facility’s vaccination program (monitor progress and initiate vaccination orders) Management: • Improve staff/management retention through efficient training • Designate managers to oversee specific clinical areas (anemia, vascular access, infection, adequacy,
Hold QAPI meetings at least monthly to discuss patient issues and concerns and facility issues and concerns • Improve documentation, tracking and timely/accurate data submission •
Next steps of the project: Review and update your QAPI as necessary • The Network will continue monitoring your facility’s SMR for the next 3 years • Review your facility’s DFR to ensure the data reported is correct •
Svetlana (Lana) Kacherova, QI Director skacherova@nw 18. esrd. net Lisle Mukai, QI Coordinator lmukai@nw 18. esrd. net 6255 Sunset Boulevard Suite 2211 Los Angeles CA 90028 (323) 962 -2020 (323) 962 -2891/Fax www. esrdnetwork 18. org