The Healthcare Association of New York State Inpatient


 –")
 – Completed only on Medicare Part A patients – 3")






 - admission –")









 n Costs = Charges *")




 provides specific billing instructions (can download")






- Slides: 42
The Healthcare Association of New York State Inpatient Rehabilitation Facility Prospective Payment System IRF PPS Mark Callan, Vice President Kelly Price, Principal Analyst October 2001
Background – Inpatient rehabilitation units/hospitals excluded from inpatient PPS - 1983 – BBA, BBRA and BIPA -legislated IRF PPS – November 3, 2000 – Proposed rule published in Federal Register – Comments to CMS on scope of PPS, patient assessment tool, and use of modifiers to adequately address costs of care – April 20, 2001 – CMS revised instrument – August 7, 2001 – Final Rule published
New Language – CMS- Centers for Medicare and Medicaid Services ( formerly HCFA) – PAI – Patient Assessment Instrument – RIC – Rehabilitation Impairment Category – CMG – Case Mix Group – FIM – Functional Independence Measure – ADL – Activities of Daily Living
Patient Assessment Instrument (PAI) – Completed only on Medicare Part A patients – 3 page form-both payment and research items – Uses modified version of Functional Independence Measure (FIMTM) from UDSmr – Completed as a routine on admission and discharge* – ARD- Sets Assessment reference date – CMG – generated by form completion – Some assessments are required by CMS under special circumstances
Anatomy of a CMG Impairment Group Code Comorbidities FIM Scores Age CMG
IRF PPS Data Transmission n Assuring minimum available hardware requirements 133 MHZ or faster -Pentium compatible CPU w/ CD-ROM; 32 megs RAM; Web browser w/ 128 bit SSL encryption ( e. g. Navigator 4. 08) Establish secure data entry account n Software for routine data entry n Coordination with billing n Maintain integrity of systems and records n
Reimbursement
Scope Includes: n Operating Costs n Capital Costs Not Included: n DME n Bad Debts
Phase-In n Cost Reports beginning between January 1, 2002 and September 30, 2002 - payment = 1/3 TEFRA + 2/3 PPS OR 100% PPS Election must be received 30 days before start of CRP For Jan. 1 hospitals = December 1, 2001 n Cost Reports beginning on or after October 1, 2002 - payment = 100% PPS
National Rate = $11, 838 n n n FFY 1996, 1997, & 1998 cost report data CY 1998 & 1999 Medicare claims with available FIM data Payment data for 1, 024 facilities FIM and claim data for ~74% of MEDPAR rehab cases 1. 16% permanently carved out for Behavioral adjustment 3% carved out & reserved for payment of cost Outliers – 5% carve out would reduce National rate to ~ $11, 594 n Adjusted for case and facility level factors
Case Mix Groups n Defined by – major impairment group (RIC) - admission – Motor score, cognitive score, age - admission – Comorbidities - discharge 95 CMGs, further divided by comorbidities into 4 payment tiers n 5 Special CMGs for short stays and expired cases n Total of 385 unique payment rates n Complete grouping rules for PAI Instrument not explicitly listed anywhere but can be inferred from IRVEN software n
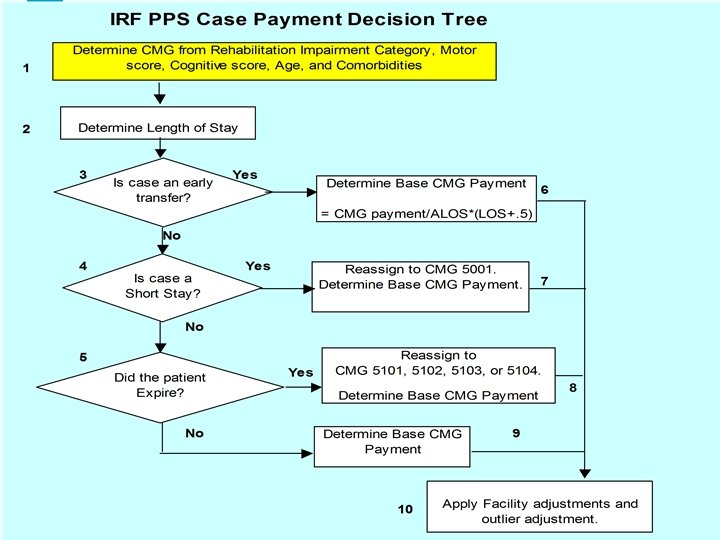
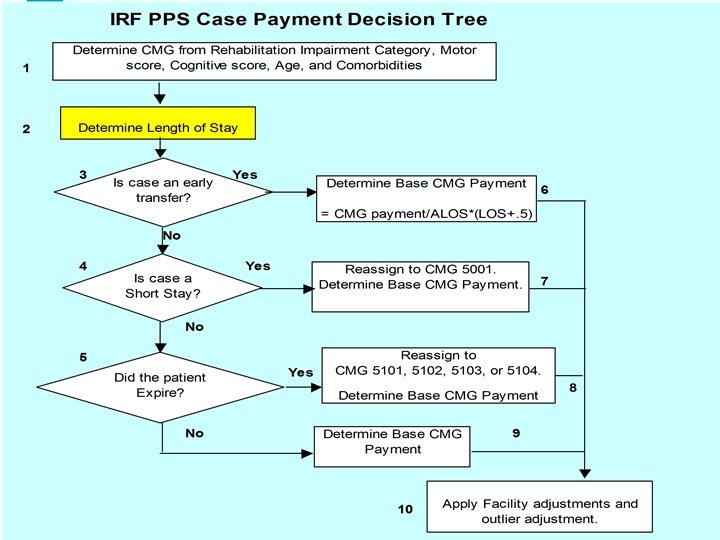
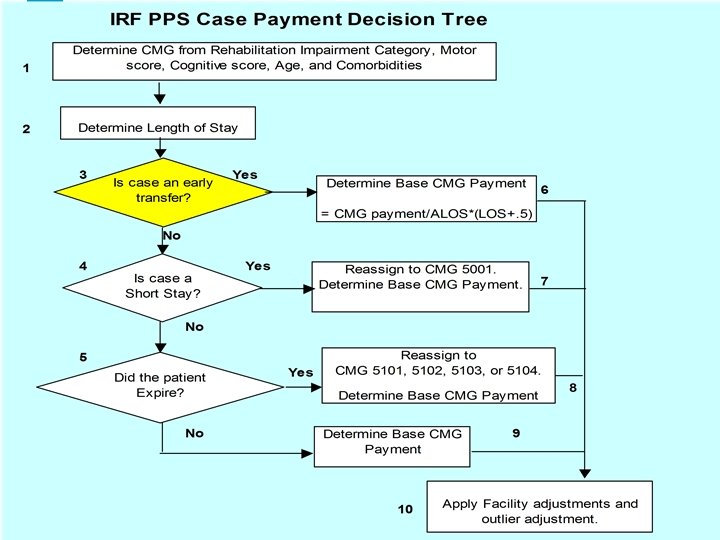
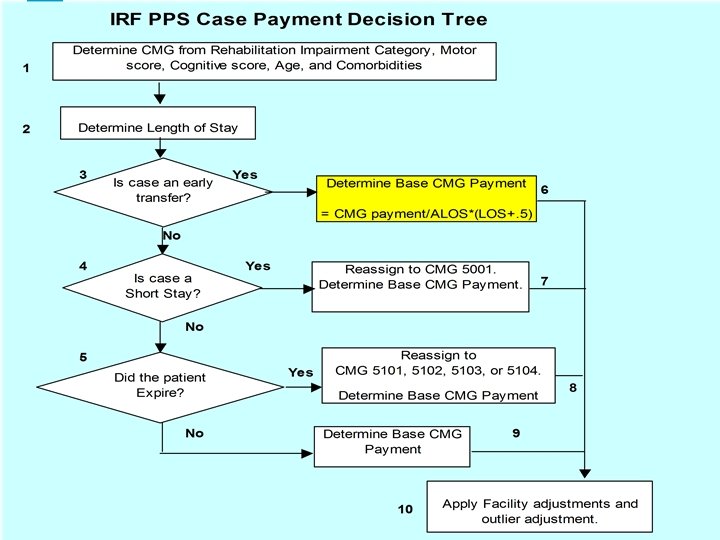
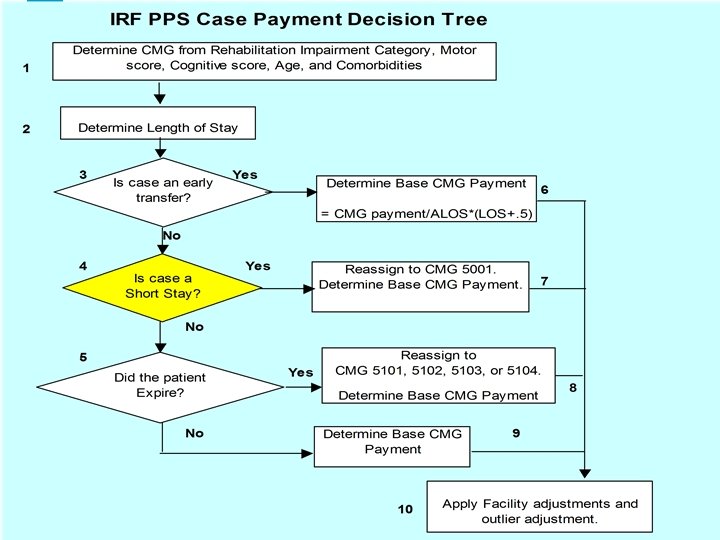
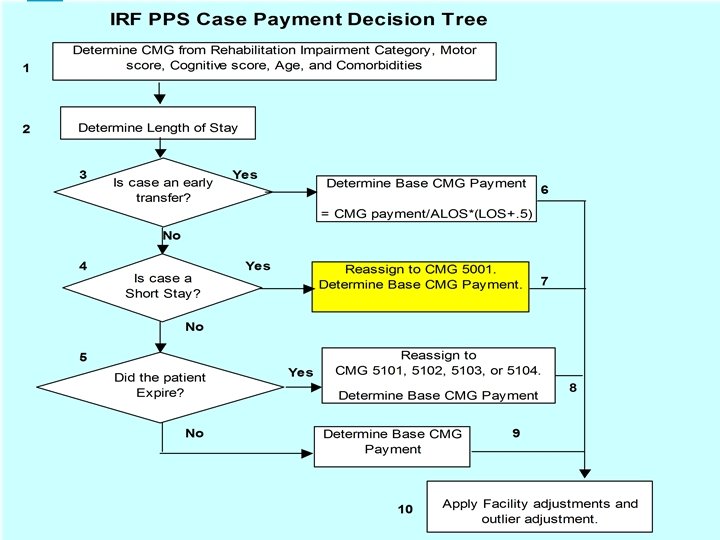
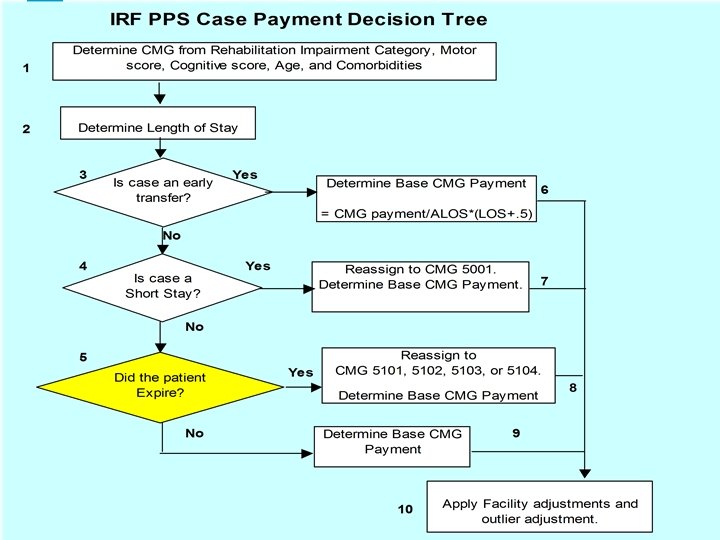
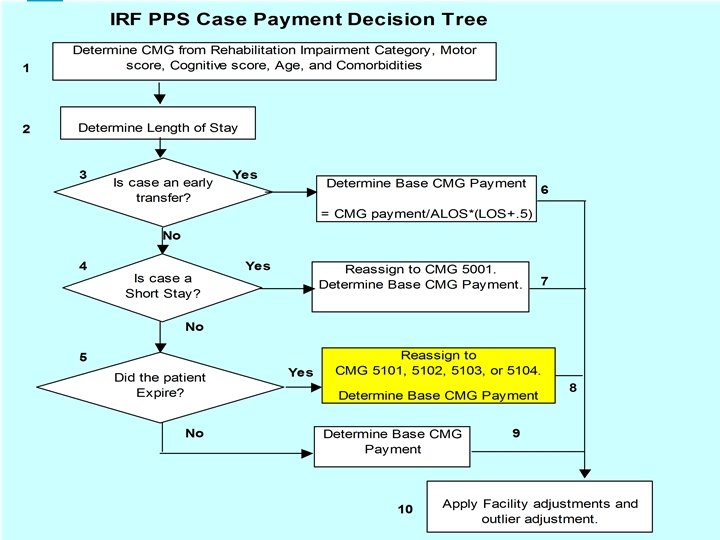
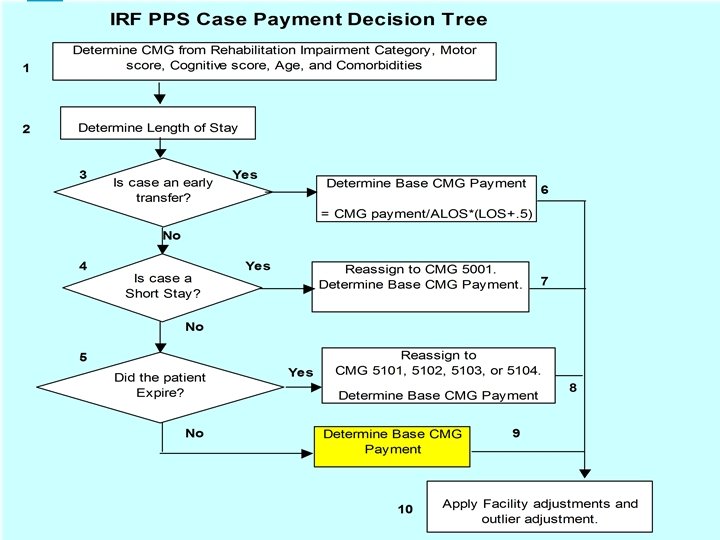
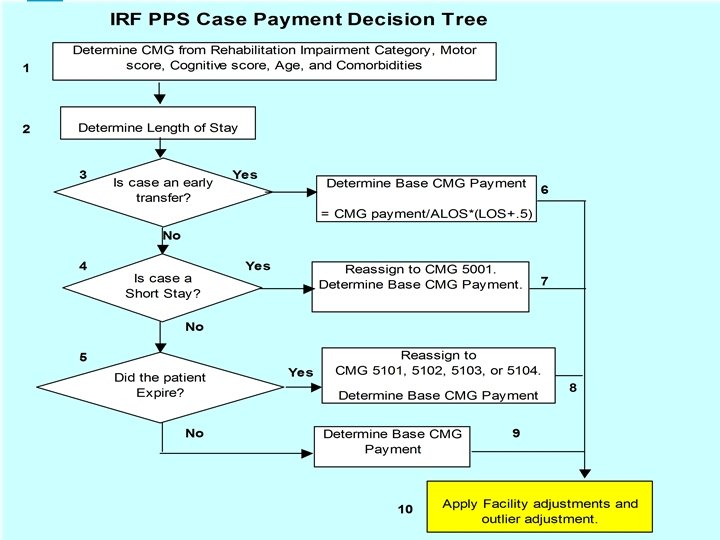
Case Level Adjustments Flow Chart n Interrupted stay n Early Transfers n Short Stay n Expired n Cost Outliers
Interrupted Stay n patient is discharged & returns by midnight of Day 3 (day of discharge = Day 1) n Ignore initial discharge assessment n Continue with same assessment instrument n Paid as a single discharge n LOS is reduced by the interruption
Early Transfer Cases of Stay < ALOS for CMG n Discharged to n Length – Another rehabilitation facility – A long-term care hospital – An inpatient hospital – A nursing home n Paid a per-diem based on CMG payment plus ½ day for up-front costs
Short Stay – CMG 5001 n Length of Stay <= 3 days n Payment = $1, 954. 45 plus facility adjustments
Expired Cases CMG 5101 Orthopedic RIC <= 13 Days CMG 5102 Orthopedic RIC >13 Days CMG 5103 Non-Orthopedic RIC <= 15 Days CMG 5104 Non-Orthopedic RIC >15 Days
Facility Level Adjustments n Wage Index n Low Income Patient percentage n Rural location
Wage Index No rural floor, no reclassifications TEFRA 1998 Hospital wage data 60% of teaching salaries removed IRF PPS 1997 Hospital wage data 100% of teaching salaries removed
Low-Income Patient Adjustment n rehab specific SSI % n rehab specific Medicaid % n LIP = (1+SSI % + Medicaid%)^. 4838 – (1+. 04+. 16)^. 4838=1. 0922 n average adjustment more rational – 5% of $11, 838 - final – 90% of $6, 024 - proposed
Rural Facility Adjustment n Applies to any facility in a non-MSA n Payment = (CMI, Wage, and LIP adjusted payment)* 1. 1914
Cost Outlier n Paid 80% of (Costs – Threshold) n Costs = Charges * RCC n Threshold = ((CMG payment + $11, 211)*facility adjustments)
Payment Example – Standard CMG 1005 with a Tier 1 Comorbidity Case-Mix Index 1. 7588 CMI adjusted Rate $20, 821 $11, 838 x 1. 7588 = Wage Index (WI) 0. 8472 Labor Portion of CMI Adjusted Rate $20, 821 x. 72395 = $15, 073 WI adj. Labor Portion $15, 073 x 0. 8472 = $12, 770 WI Adjstd Labor + Non-Labor Portion $12, 770 + (0. 27605 x $20, 821) = $18, 518 LIP Adjustment 1. 0922 x $18, 518 = $20, 225 Rural Adjustment 1. 1914 x $20, 225 = $24, 096
Payment Example – Outlier CMG 1005 with a Tier 1 Comorbidity Fixed Loss Amount $11, 211 Wage Index (WI) 0. 8472 WI Adjusted Fixed Loss Amount $9, 971 LIP Adjustment 1. 0922 x $9, 971 = $10, 890 Rural Adjustment 1. 1914 x $10, 890 = $12, 975 Outlier Threshold Cost for Case Outlier Payment $12, 975 + $24, 096 = $37, 070 $50, 000 80% * ($50, 000 - $37, 070) = $10, 344
Payment Example – Transfer CMG 1005 with a Tier 1 Comorbidity Discharge Destination Code 05 = Skilled Nursing Facility Average Length of stay for CMG 1005 Actual Length of Stay Fully adjusted CMG Rate Average Daily Payment Actual Length of Stay plus ½ day Transfer Case Payment 21 7 $24, 096 $1, 147 7. 5 $8, 606
CMS Impact Estimates Full Implementation Nation n Freestanding n Hospital Units n Teaching n +0% -4% +2% +0% – Resident to ADC 10%=19% -3% – Resident to ADC>19% -2% n Non-Teaching +0% – Resident to ADC<10%
Billing Information CMS Program Memorandum A-01 -110 (9/14/01) provides specific billing instructions (can download from CMS site). n Items that must be entered on the bill include: Revenue Code 0024 5 digit HIPPS Rate/CMG Code. n Patient Status will have 2 new codes added to the list of possible status codes: 62 Discharged to another rehab facility 63 Discharged to a long-term care hospital n
HANYS Grouper/Pricer Model n Facility specific TEFRA payments vs. PPS n Facility must review TEFRA calculations n Facility must enter individual cases to estimate PPS payments n Data Edits and Information with Data Entry
Ways to Use it n Impact Estimate n Calculate payments for unusual cases n Calculate payments for groups of cases n Education and Training
PPS Payment estimate UDSmr Instrument n Availability of historic info n Not an exact grouping n Primary use is to determine whether to elect 100% PPS payment IRF PAI n Precise grouping n Training tool n Includes FIM Modifiers n Primary use is to calculate actual PPS payment.
Case Data Entry Need UDSmr assessment n Be precise in entering codes for impairment categories and comorbidities n – Print out RIC and Comorbidity appendices n Review results and decide if this is a typical case – If Yes, then Log and Clear n Enter next case
Impact Analysis n Comparison of Payments PPS vs. TEFRA n Comparison of Payments vs. Historic Cost n Per-discharge & Per-Day n Check Average Lengths of Stay – – is your sample representative?
Contact Information n If you encounter a problem while running the grouper/pricer or have any other concerns or comments, please contact either: Kelly Price (Kprice@hanys. org) (518) 431 -7729 or Lee Santos (Lsantos@hanys. org) (518) 431 -7708