Successful Percutaneous Managementof of aa Giant Saphenous Vein
")















- Slides: 17
Successful. Percutaneous. Managementof of aa. Giant. Saphenous. Vein. Graft. Aneursym Edward Howard MBCh. B(Hons) Ph. D Robert Lager MD Augusto Pichard MD Medstar Washington Hospital Center
Edward W. Howard, MD, Ph. D I/we have no real or apparent conflicts of interest to report.
The Case • 79 -year-old male, with past history of four separate coronary artery bypass grafting procedures (1980 -1991) • Presented with weight loss, hoarseness of the voice and vertigo. • Past history included hypertension, dyslipidemia, permanent atrial fibrillation, ischemic cardiomyopathy with EF of 35 -40%, mitral regurgitation • No tobacco use, mild alcohol intake. • His exam showed a comfortable, thin but not cachectic patient with pulse of 55, blood pressure of 105/54, afebrile. No other pertinent physical exam findings. • Of note: recently diagnosed with vocal cord paralysis by his ENT
Radiology
CT • • • Likely SVG pseudoaneurysm versus true aneurysm with dimensions 7. 3 x 6. 6 x 8. 7 cm Severe native coronary artery disease RIMA (supplying LAD) as well as the right ventricle with likely adhesions to the sternum Hypokinesis of the anterior wall with preserved LV ejection fraction Moderate to severe dilation of the right ventricle as well as the right and left atria.
3 D Reconstruction
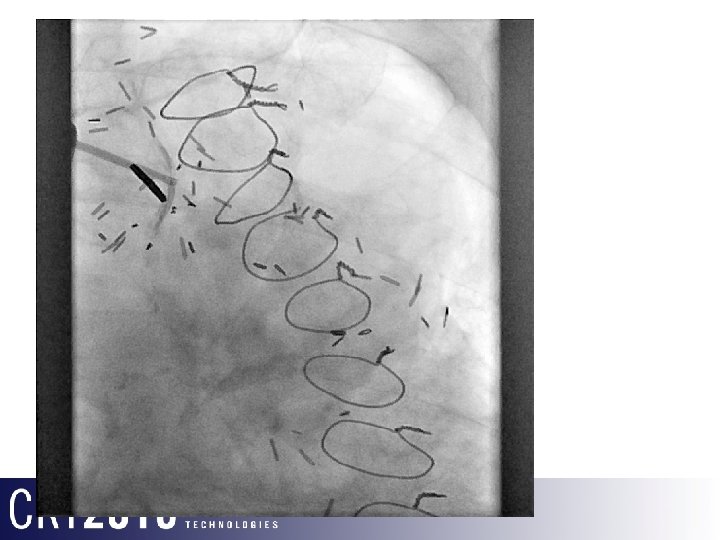
The Procedure
The Procedure
6 Month Outcome • Returned for follow up with mildly improved symptoms • CT shows patent stent, progressive thrombosis of aneurysm, regression of pulmonary arterial compression
SVG Aneurysm • First described by Riahi and colleagues in 19751 • Rare, but multiple case reports and small case series and recent narrative meta-analysis 2 • Incidence of aortocoronary SVG is reportedly 0. 07% (single institution with 5500 SVGs)3 • Appears to be increasing in prevalence • Defined as >1. 5 x dilation of vessel diameter, but >10 cm has been reported • 68% of reported aneurysms occur >10 years after surgery 1. Riahi M, Mark Vasu C, Tomatis LA. J Thoracic Cardiovasc Surg. 1975; 70: 358 – 359 2. F. Daniel Ramirez et al; Circulation, 2012; 126: 2248 -2256 3. Dieter RS et al. Cardiovasc Surg. 2003; 11: 507– 513
Pathophysiology • Delayed presentation and low incidence suggest that arterial pressures alone are not the cause of late SVG aneursym. More likely: – Atherosclerotic changes – Orientation of smooth muscle fibers at the level of the valves – Dysfunction of graft endothelium • Separate group of early presentation SVG aneursyms – – Infection Unsuspected pre-existing disease in vein conduit Factors in harvesting such as conduit injury Surgical errors such as poor suture technique and reverse implantation
Outcomes of SVG Aneurysm NOT BENIGN! SVG Aneursym Myocardial Infarction Death Rupture Compression of Adjacent Structures
Outcome by Size Proportionate to size, but no size is safe! Adapted from F. Daniel Ramirez et al; Circulation, 2012; 126: 2248 -2256
Percutaneous Management of SVG Aneurysm • Traditionally surgical • Coiling or closure devices have been used for SVGAs not supplying significant areas of viable myocardium • Covered aortic endograft has also been described as an endovascular option for SVGA occlusion. • To date, this is the largest SVGA to which this therapy has been successfully applied, suggesting it is an option for all sizes of SVGA
Questions?