Radiological Category Thoracic Chest Principal Modality 1 General
: General Radiography Principal Modality (2): Case Report")








 In this patient, the large right anteroinferior pleural air collection is contiguous")


- Slides: 20
Radiological Category: Thoracic Chest Principal Modality (1): General Radiography Principal Modality (2): Case Report #0332 Submitted by: Joy A. Henningsen, M. D. Faculty reviewer: Sandra A. A. Oldham, M. D. Date accepted: 21 July 2006 CT
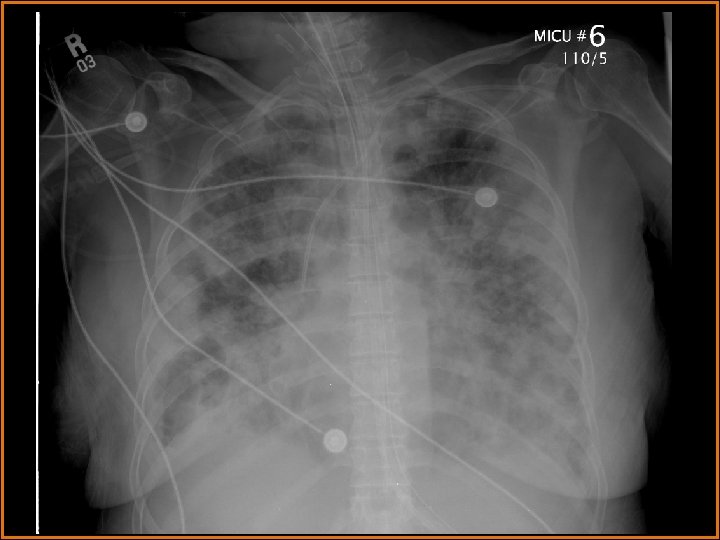
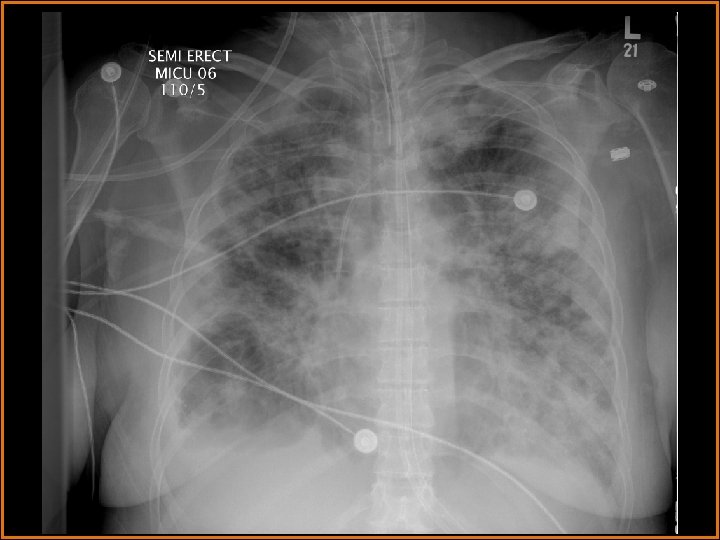
Case History 64 -year-old female presents with fever. Two serial portable chest radiographs are provided.
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • Cavitary Metastases • Multifocal Pneumonia • Septic Emboli • Wegener’s Granulomatosis • Sarcoidosis • Multiple Pulmonary Infarcts • Pneumothorax • Primary Bronchogenic Carcinoma
Findings and Differentials Chest x-ray findings: Multiple bilateral patchy alveolar opacities are seen diffusely. Many of these opacities are nodular, and some are cavitary. There are bilateral pleural effusions. Retrocardiac opacification is seen and may be secondary to the effusions and/or the airspace disease. The life support lines and tubes are unremarkable. A large lucency projects over the right hemidiaphragm. What would you like to do next? Think about your answer before advancing to the next slide.
Radiological Presentations
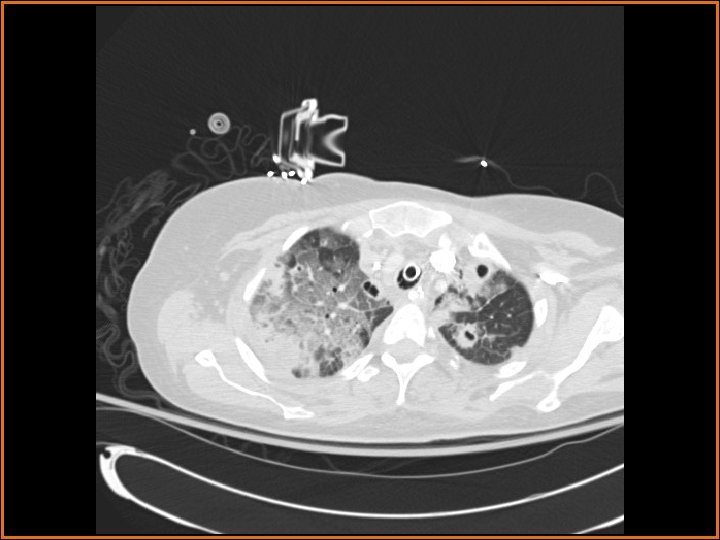
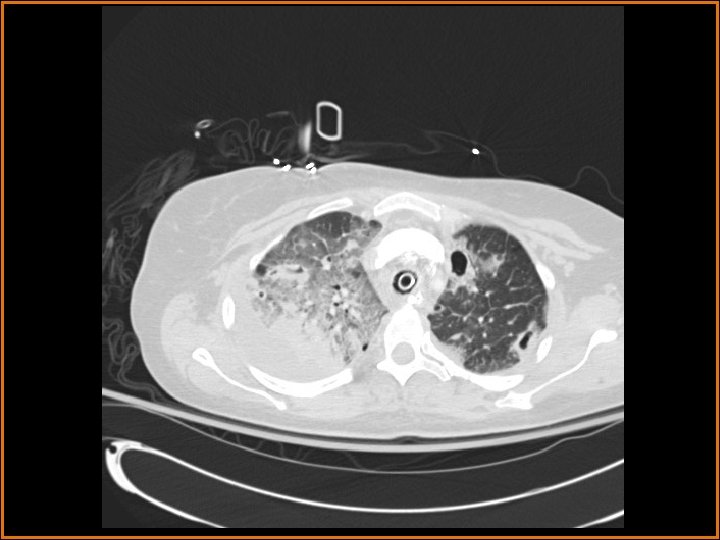
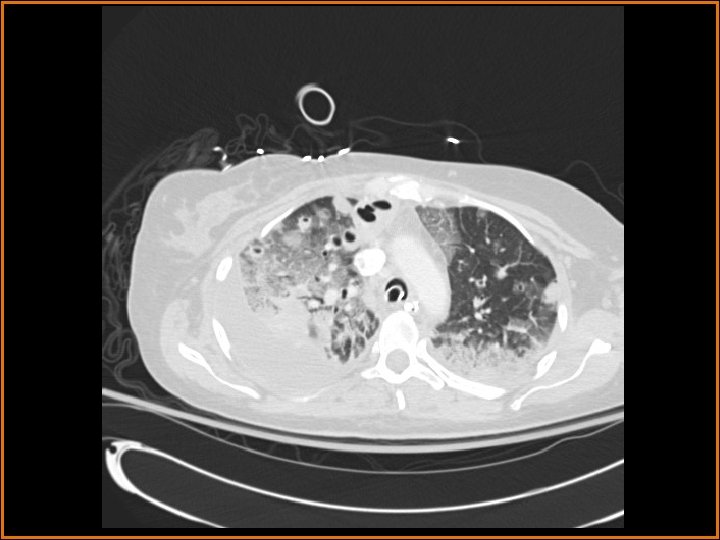
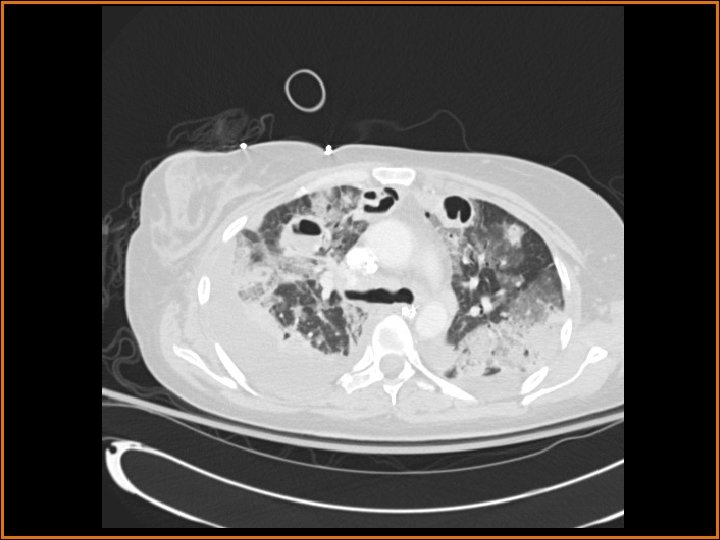
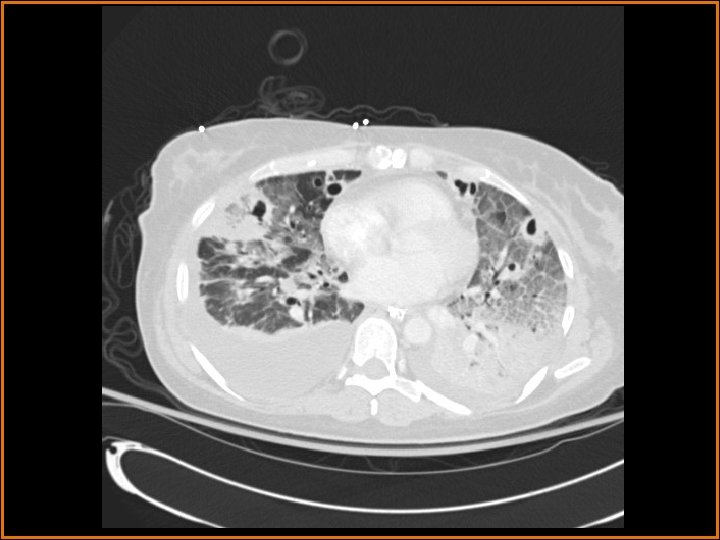
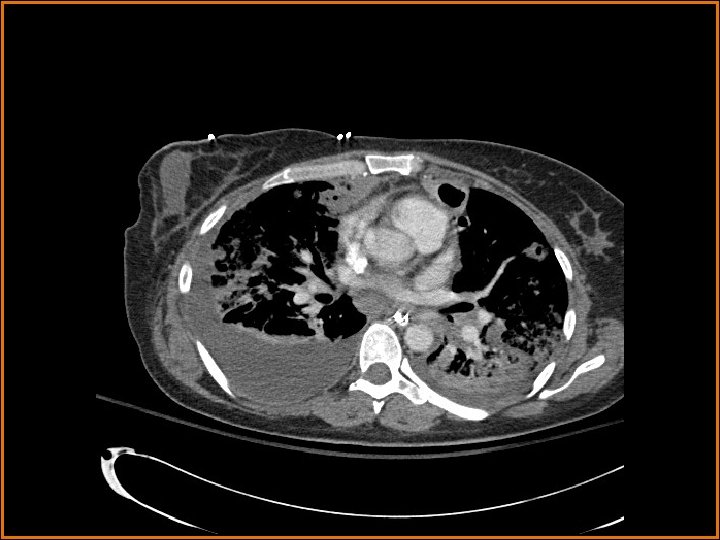
Findings and Differentials CT Findings: Multiple bilateral peripheral nodular opacities are seen, many of which are fed by arterial branches. Some of the nodules are cavitary. Diffuse bilateral ground glass opacities are seen with air bronchograms. The large lucency projecting over the right hemidiaphragm on the plain film corresponds to a pleural air collection that is directly contiguous with one of the cavities. Differential Diagnosis: • Multiple cavitary metastases • Septic Emboli
Discussion The differential diagnosis of cavitary nodules includes cavitary metastases, septic emboli, fungal infections, rheumatoid nodules, Wegener's granulomatosis, and rheumatoid nodules, among others. In this patient with fever, an infectious or inflammatory etiology is at the top of the differential. Correlation of the history with the imaging findings supports the diagnosis of septic emboli. Septic emboli usually manifest as multiple, bilateral peripheral opacities which may or may not cavitate. Often, the emboli will be in different stages of cavitation. Demonstration of a feeding vessel into the nodules indicates the hematogenous etiology of this process (although hematogenous metastases and a small-vessel vasculitis could certainly exhibit this feature also). Septic emboli may lead to pulmonary infarctions, which are seen as wedge-shaped opacities abutting the pleural surface, with the apex of the triangle pointing away from the pleura. The periphery of the infarct can enhance, but the center usually does not. Distinguishing infarcts from pneumonia is made easier when a vessel can be seen terminating at the apex of the infarcted region. (CONTINUED ON NEXT SLIDE)
Discussion (Continued) In this patient, the large right anteroinferior pleural air collection is contiguous with one of the cavities (as seen on the second CT image) and represents a bronchopleural fistula. Etiologies of bronchopleural fistulas include necrotizing infection, active TB, irradiation, tumor in a bronchial margin, etc. If the bronchopleural fistula is large, a persistent pneumothorax with or without contralateral mediastinal shift may be present. In this case, a septic embolus had eroded into the pleural space, creating the lucent collection projecting over the right hemithorax on the plain films. Finally, the ground glass opacities represented pneumonia in this patient.
Diagnosis Septic Emboli with Bronchopleural Fistula
References Webb, W et al. High-Resolution CT of the Lung. 3 rd Ed. Philadelphia: Lippincott, Williams, & Wilkins. 2001. Weissleder, R et al. Primer of Diagnostic Imaging. 3 rd Ed. Philadelphia: Mosby. 2003.