Radiological Category Thoracic Chest Principal Modality 1 General
: General Radiology Principal Modality (2): CT Case")








- Slides: 11
Radiological Category: Thoracic Chest Principal Modality (1): General Radiology Principal Modality (2): CT Case Report #0023 Submitted by: Huan Nguyen, M. D. Faculty reviewer: Sandra A. A. Oldham, M. D Date accepted: 26 November 2003
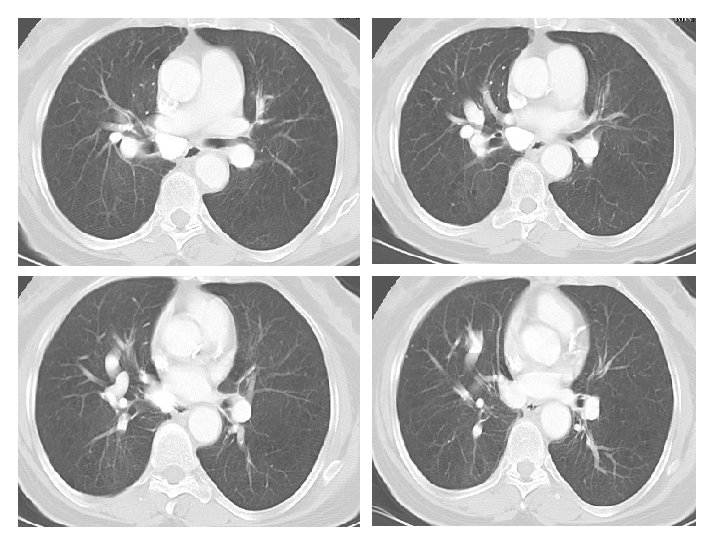
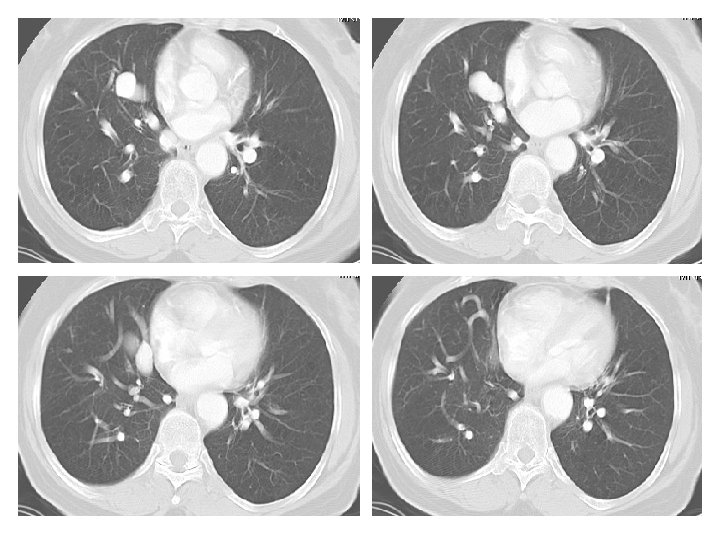
Case History 65 year old male with shortness of breath. Images: PA and Lateral View of the chest. CT of the Chest with IV contrast presented in lung windows. Please note that the images proceed from left to right and top to bottom.
Radiological Presentations 104487887
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • • • Bronchiectasis Pulmonary AVM Allergic Bronchopulmonary Aspergillosis Total Anomalous Pulmonary Venous Return Scimitar Syndrome
Findings and Differentials Findings: The frontal view of the chest shows multiple prominent tubular structures arising from the right hilum and coursing inferiorly adjacent to the right heart border. There are multiple dilated tubular structures seen in the right lung on CT. Tubular structures within the lung are either vascular or bronchial. If bronchial, they would have to be filled with inspissated mucus to be opaque. But there are bronchi seen adjacent to these tubular structures and the bronchi are normal. The tubular structures therefore represent dilated pulmonary arteries and veins. The remainder of the right lung is normal. There also several calcified lymph nodes from prior granulomatous disease. The cardiac silhouette is normal. There are no pleural effusions. Differential: • Total Anomalous Pumonary Venous Return • Pulmonary AVM • Scimitar Syndrome
Discussion These findings are diagnostic of pulmonary AVMs are believed to be congenital defects in the terminal capillary loops that result in dilatation and formation of vascular sacs. 40 -65 percent of patients with pulmonary AVMs also have AVMs elsewhere (skin, CNS, solid organs). AVMs are seen in Osler-Weber-Rendu disease. Pumonary AVMs appear on imaging as vascular masses adjacent to the pleura or the bronchovascular bundles. They are common in the lower lobes. The draining veins are usually larger in size compared to the feeding arteries. They usually do not cause symptoms but can cause hemoptysis. Due to the right to left shunting, pulmonary AVMs are associated with cerebral abscesses. The right to left shunting also decreases the Pa. O 2 and causes the cardiac output to increase. Angiography is seldom needed to diagnose the condition. The CT findings of multiple dilated pulmonary vessels clinches the diagnosis. It is important to show the feeding artery and draining vein. Catheter embolization is the preferred treatment modality. Dilated bronchi filled with inspissated mucus can mimic this condition.
Discussion Scimitar syndrome consists of a hypoplastic right lung, small right hilum and an anomalous prominent curving vessel (mimics a Turkish sword called a scimitar) adjacent to the right heart border taking blood below the diaphragm, usually to the IVC (partial anomalous pulmonary venous return). This creates a left to right shunt.
Diagnosis Pulmonary Arteriovenous Malformation