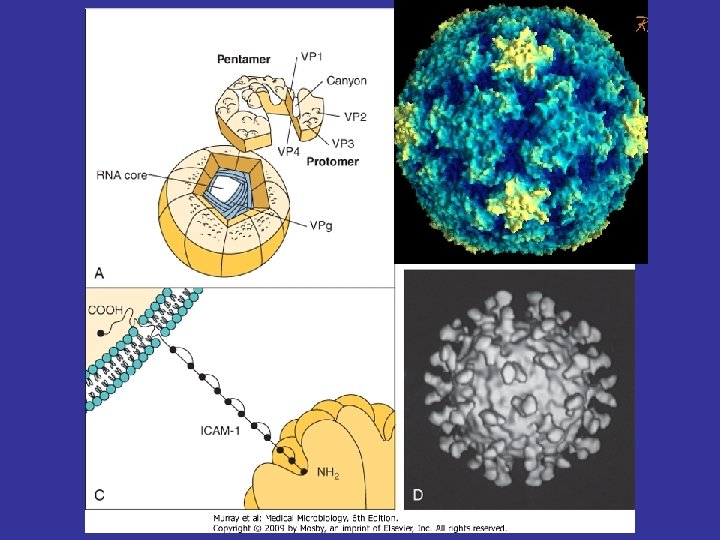
Picornavirus Pico RNA Picorna Virion is a naked

 icosahedral capsid enclosing")


 The initiation AUG codon in the polio virus")









 meningitis • Coxsackie A, B • Echovirus • Summer and fall")





- Slides: 29
Picornavirus Pico + RNA = Picorna
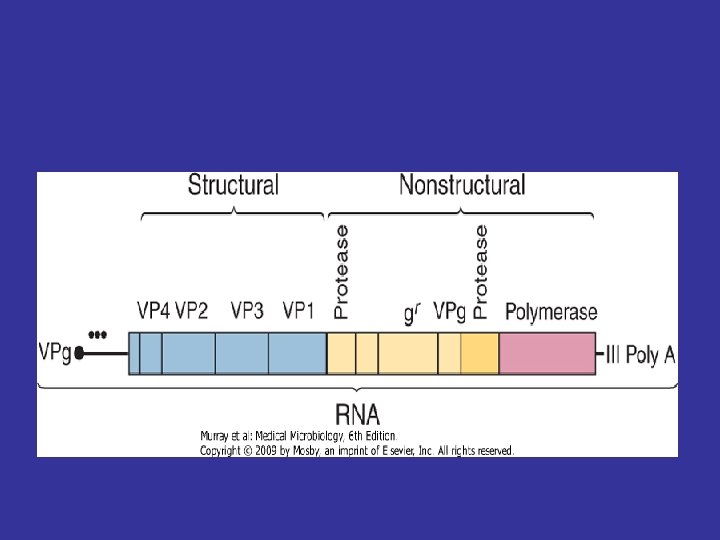
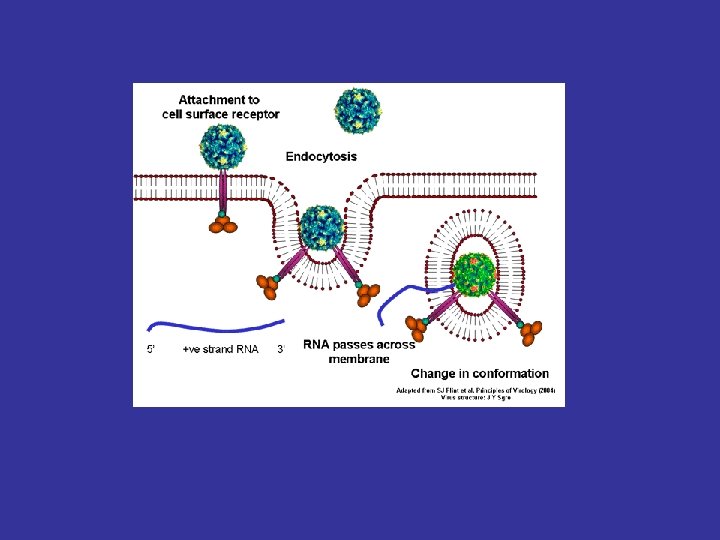
• Virion is a naked, small (25 to 30 nm) icosahedral capsid enclosing a single-stranded positive RNA genome. Box 56 -2. Unique Properties of Human Picornaviruses • Enteroviruses are resistant to p. H 3 to p. H 9, detergents, mild sewage treatment, and heat. • Rhinoviruses are labile at acidic p. H; optimum growth temperature is 33° C. • Genome is an m. RNA. (+ sense) • Naked genome is sufficient for infection. • Virus replicates in cytoplasm. • Viral RNA is translated into polyprotein, which is then cleaved into enzymatic and structural proteins. • Most viruses are cytolytic
Picornaviridae • Enterovirus • Poliovirus types 1, 2, and 3 • Coxsackie A virus types 1 to 22 and 24 • Coxsackie B virus types 1 to 6 Body_ID: B 056001 • Echovirus (ECHO virus) types 1 - 9, 11 - 27, 29 - 34 • Enterovirus 68 to 71 and 73 to …. • Parechovirus (formerly echovirus 22, 23) • Kobuvirus: Aichi virus and Ljungan virus • Hepatovirus -Hepatitis A virus • Rhinovirus types 1 to 100+ Animal viruses: • Cardiovirus • Aphthovirus ….
• e. IF 4 G cleaved cellular protein synthesis is shut off
Kozak sequence (NNNPu. NNA UGG ) The initiation AUG codon in the polio virus open reading frame is preceded by eight other AUGs. RCCAUGG RYYAUGG (R = purine, Y = pyrimidine);
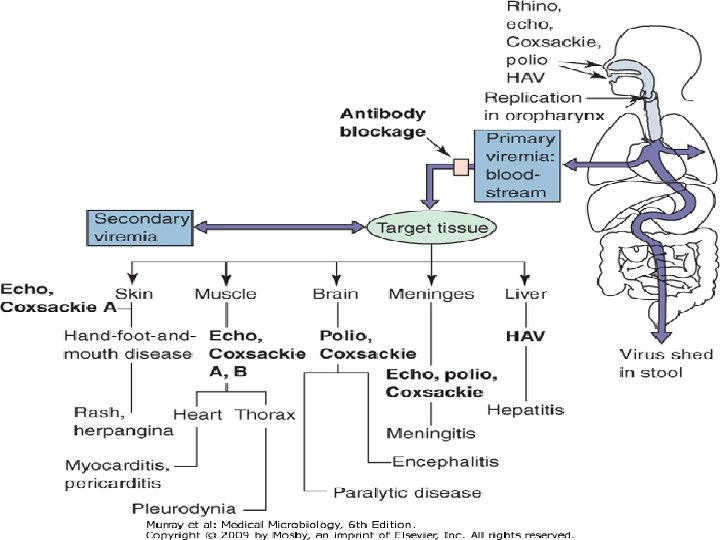
Disease Mechanisms of Picornaviruses • Enteroviruses enter via the oropharynx, intestinal mucosa, or upper respiratory tract and infect the underlying lymphatic tissue; rhinoviruses Body_ID: B 056003 are restricted to the upper respiratory tract • In the absence of serum antibody, enterovirus spreads by viremia to cells of a receptor-bearing target tissue • Different picornaviruses bind to different receptors, many of which are members of the immunoglobulin superfamily (i. e. , ICAM-1) • The infected target tissue determines the subsequent disease • Viral, rather than immune, pathologic effects are usually responsible for causing disease symptoms • The secretory antibody response is transistory but can prevent the initiation of infection • Serum antibody blocks viremic spread to target tissue, preventing symptoms • Enterovirus is shed in feces for long periods • Infection is often asymptomatic or causes mild, flulike or upper respiratory tract disease
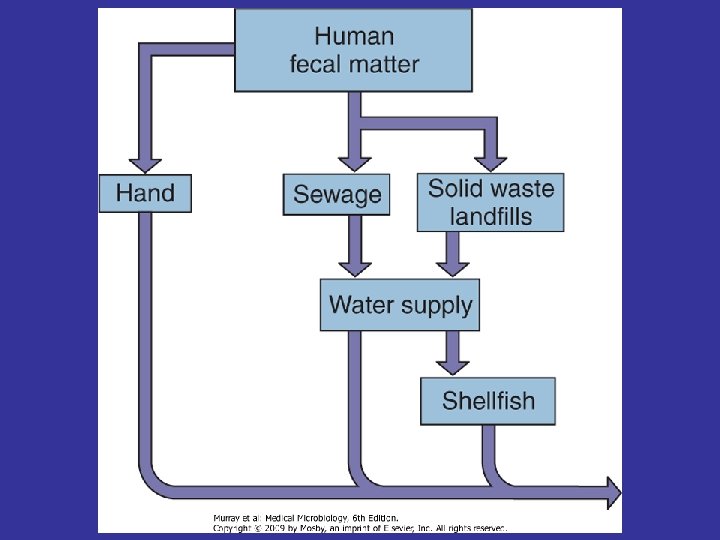
Epidemiology of Enterovirus Infections Disease/Viral Factors • Nature of disease correlates with specific enterovirus and age of person • Infection often asymptomatic, with viral shedding • Virion resistant to environmental conditions (detergents, acid, drying, mild sewage treatment, and heat) Transmission • Fecal-oral route: poor hygiene, dirty diapers (especially in daycare settings) • Ingestion via contaminated food and water • Contact with infected hands and fomites • Inhalation of infectious aerosols Body_ID: B 056004 Body_ID: PB 056004
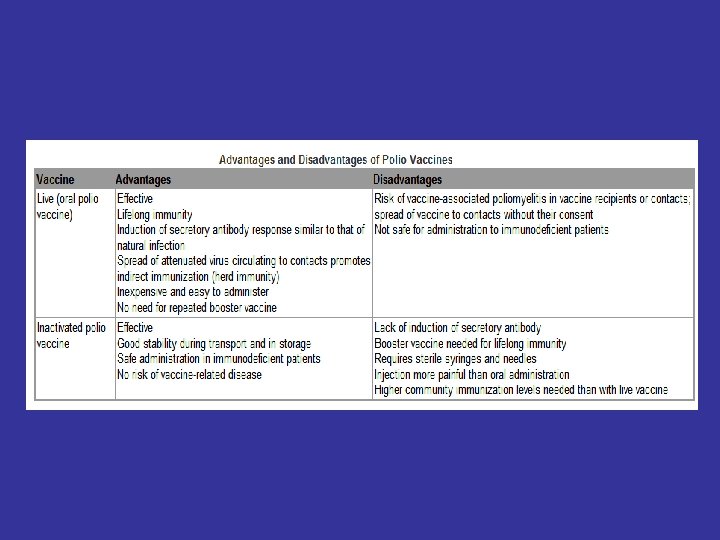
Who Is at Risk? Body_ID: B 056004 • Young children: at risk for polio (asymptomatic or mild disease) • Older children and adults: at risk for polio (asymptomatic to paralytic disease) • Newborns and neonates: at highest risk for serious coxsackievirus and enterovirus disease Geography/Season • Viruses have worldwide distribution; wild-type polio virtually eradicated in developed countries because of vaccination programs • Disease more common in summer Modes of Control Body_ID: PB 056004 • For polio, live oral polio vaccine (trivalent OPV) or inactivated trivalent polio vaccine (IPV) is administered • For other enteroviruses, no vaccine; good hygiene limits spread
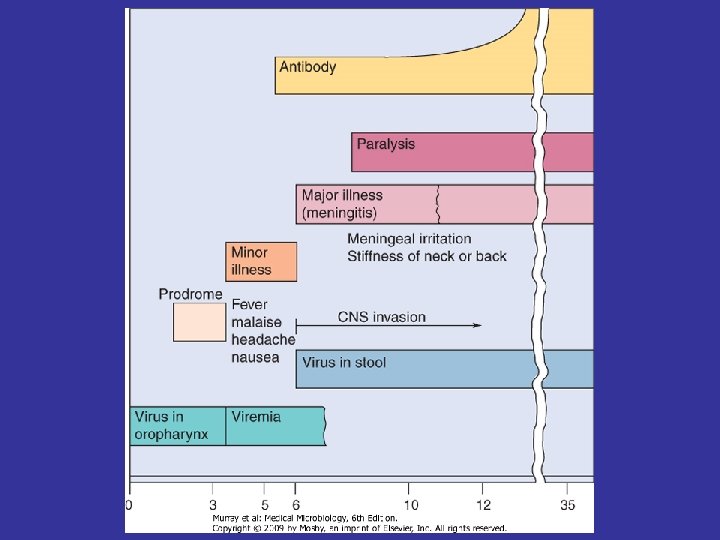
Poliovirus infection • • • Asymptomatic illness results if the viral infection is limited to the oropharynx and the gut. At least 90% of poliovirus infections are asymptomatic. Abortive poliomyelitis, the minor illness, is a nonspecific febrile illness occurring in approximately 5% of infected people. Fever, headache, malaise, sore throat, and vomiting occur in such people within 3 to 4 days of exposure. Nonparalytic poliomyelitis or aseptic meningitis occurs in 1% to 2% of patients with poliovirus infections. In this disease, the virus progresses into the central nervous system and the meninges, causing back pain and muscle spasms in addition to the symptoms of the minor illness.
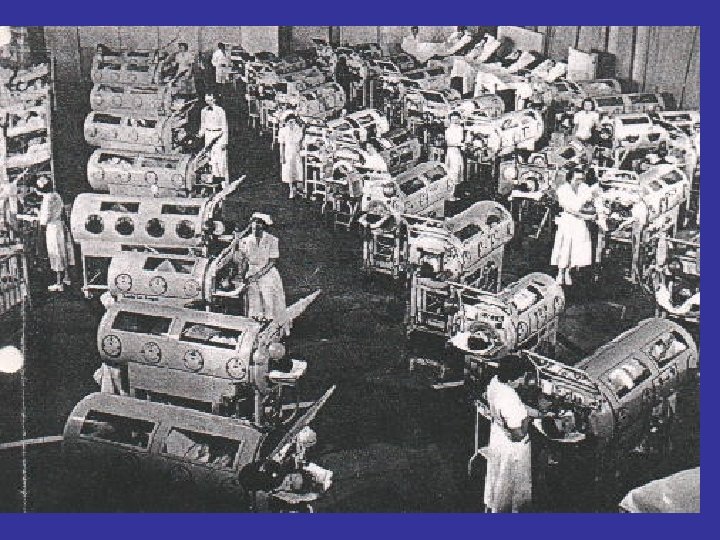
• Paralytic polio, the major illness, occurs in 0. 1% to 2. 0% of persons with poliovirus infections and is the most severe outcome. It appears 3 to 4 days after the minor illness has subsided, thereby producing a biphasic illness. In this disease, the virus spreads from the blood to the anterior horn cells of the spinal cord and to the motor cortex of the brain. The severity of paralysis is determined by the extent of the neuronal infection and by which neurons are affected. Spinal paralysis may involve one or more limbs, whereas bulbar (cranial) paralysis may involve a combination of cranial nerves and even the medullary respiratory center. • Paralytic poliomyelitis is characterized by an asymmetrical flaccid paralysis with no sensory loss. Poliovirus type 1 is responsible for 85% of the cases of paralytic polio. Reversion of the attenuated vaccine virus types 2 and 3 to virulence can cause vaccine-associated disease.
Coxsackievirus and Echovirus Infections
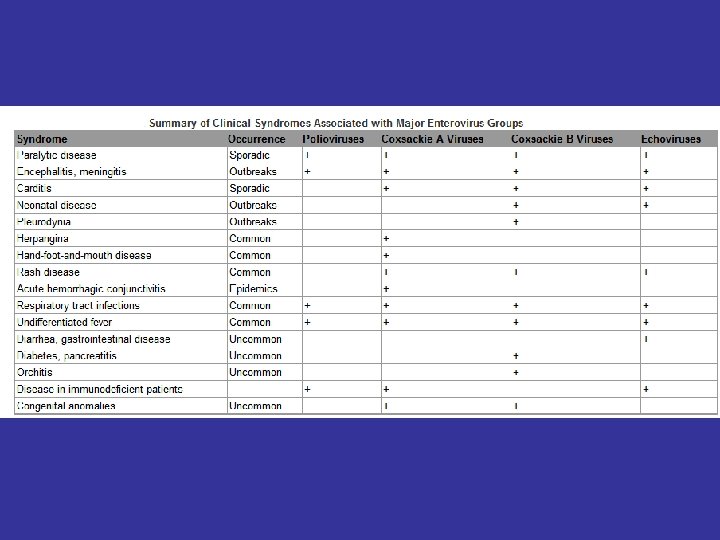
• Herpangina Type A 1 -10 Type B 1 -5 Echoviruses Mostly in children; epidemicin summer months Abrupt fever, sore throat, anorexia, abdominal pain and vesicles on soft palate, pharinx and tonsills
Hand-foot-and-mouth disease • Coxsackie A 16, 4, 5, 10
Myocardial and pericardial infections • Coxsackie B, echovirus • Sudden onset Diabetes: Coxsackie B 4
Viral (aseptic) meningitis • Coxsackie A, B • Echovirus • Summer and fall
Fever, rash, and common coldlike symptoms • Summer minor illnes: Rubelliform rush on face, neck and chest Accompanied by fever No distinctive feature Short duration
Plerodynia • Coxsackie B • Sudden chest pain, fever, malaise • (Abdominal or testicular pain)
Laboratory Diagnosis • CSF findings • Culture • Molecular and serological methods
Treatment and Prevention • Vaccine available only for Polio
Rhinoviruses • • • • Epidemiology of Rhinovirus Infections Disease/Viral Factors Virion is resistant to drying and detergents Multiple serotypes preclude prior immunity Replication occurs at optimum temperature of 33° C and cooler temperatures Transmission Direct contact via infected hands and fomites Inhalation of infectious droplets Who Is at Risk? People of all ages Geography/Season Virus found worldwide Disease more common in early autumn and late spring Modes of Control Washing hands and disinfecting contaminated objects help prevent spread