Paraquat intoxication INTRODUCTION n Paraquat 1 1 dimethyl4

 (since 1962) n completely denatured")


 found in the body.")
")





")






- Slides: 22
Paraquat intoxication
INTRODUCTION — n Paraquat (1, 1 -dimethyl-4, 4'-bipyridylium chloride) (since 1962) n completely denatured upon contact with the earth
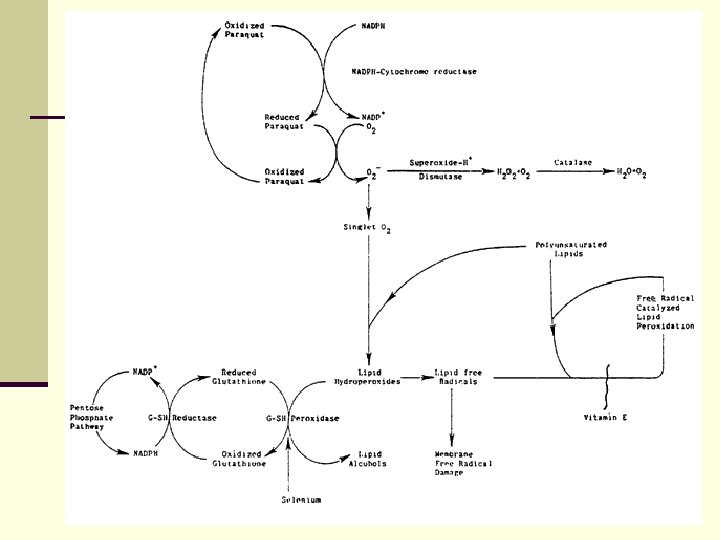
TOXICITY AND METABOLISM — n herbicidal activity : by inhibiting the reduction of NADP to NADPH during photosynthesis → superoxide, singlet oxygen, hydroxyl, and peroxide radicals → destroy lipid cell membranes by polymerization of unsaturated lipid compounds → oxidative destruction → recruitment of inflammatory cells → late and irreversible pulmonary fibrosis
In Vivo n pulmonary toxicity : highest oxygen tensions (alveoli) found in the body. n kidney toxicity : acute tubular necrosis (within 24 hours) → enhancing overall toxicity. n 口服的巴拉刈僅有5到 10%會經由腸胃道被吸 收,其餘部分由糞便排出。 n 巴拉刈於腸胃道的吸收相當快速,約於 0. 5至 2 小時內即達到血中濃度的高峰
ameliorate the toxic effects of paraquat: n deferoxamine (Complexes with trivalent ions (ferric ions) to form removal of iron) : Lipid peroxidation may be enhanced by iron radicals. n Vitamin E (a potent antioxidant) : only in cultured cells ; no clinical effect n Exogenous glutathione and n-acetylcysteine, a donor of glutathione, may protect against injury. n Sulfite or thiosulfite (redox agents) (reversing oxidized glutathione). ferrioxamine, removed by the kidneys
CLINICAL EXPOSURE — n Skin and lungs —infrequently results in systemic toxicity 0. 4 percent of a topical dose was absorbed from an unoccluded site; 1. 4 percent was absorbed from an occluded site; and 3. 8 percent was absorbed from an occluded and damaged dermal site [13]. thermal-dependent conversion of paraquat to non-toxic bipyridines. n GI tract —cause systemic toxicity + direct injury to the gastrointestinal tract
CLINICAL TOXICITY — n due to absorption via the gastrointestinal tract. n Direct local toxicity n Systemic toxicity — results from the oral ingestion
Direct local toxicity n GI tract — result from the caustic properties of paraquat: 1. Within a few minutes to hours → a burning sensation in the buccal cavity. 2. within one to two days → Ulceration of the lips, tongue, and pharynx ("pseudomembrane") → esophageal perforation. n Skin — skin rashes (particularly on scrotal and intergluteal areas), cracked nails, and epistaxis n Lungs —hemoptysis. n Eyes — Corneal ulceration and scarring.
Systemic toxicity — results from the oral ingestion n Ingestion of moderate amounts — oral ingestion of amounts of paraquat approximately between 4 to 30 m. L/kg of the liquid concentrate: n Ingestion of massive amounts — greater than 30 m. L/kg or 50 m. L of concentrate.
Ingestion of moderate amounts — n Buccal and/or esophageal ulcerations. n Renal failure (within two to six days) - Proximal tubule dysfunction. n Metabolic acidosis-- ∵myocardial failure (myocarditis+ epicardial hemorrhage with arrhythmias), adrenal gland insufficiency (due to necrosis), systemic hypotension, severe hypoxemia, and/or renal failure.
Ingestion of moderate amounts — n Pulmonary edema (24 to 48 hours after ingestion) → adult respiratory distress syndrome (first week after ingestion) : diffuse consolidation, pneumomediastinum with or without pneumothorax and subcutaneous emphysema, and cardiomegaly with widened superior mediastinum→ pulmonary fibrosis. n 喘的出現時間相對上會較晚,約在中毒後第 3至 14天才 逐漸出現 n Death usually occurs within one to two weeks, but may be observed up to six weeks after ingestion.
LABORATORY DETECTION — n A qualitative urine test for paraquat : concentrations of 1 mg/m. L or above (1 ppm) n Gas chromatography and high pressure liquid chromatography : levels of 0. 1 to 0. 2 mg/d. L. n Radioimmunoassay : levels well below 0. 1 mg/m. L. n Association with prognosis — n Fatal outcomes : plasma levels > 0. 2 mg/m. L at 24 hours after ingestion / 0. 1 mg/m. L at 48 hours.
TREATMENT — n Prevention of gastrointestinal absorption — n Removal from blood —ineffective in removing paraquat → maintenance of renal function n Ancillary treatment —
Prevention of gastrointestinal absorption — n Gastric lavage : performed cautiously in view of possible ulceration of the pharynx and the esophagus diatomaceous clays(=bentonite + Fuller's earth 30% suspension)+ magnesium sulfate, to produce a catharsis. bentonite in a 6 to 7. 5 percent suspensions of activated charcoal the ion-exchange resin sodium resonium (Kayexalate®) n Total gut lavage n polyethylene glycol solutions for bowel irrigation
Removal from blood —maintenance of renal function n Extracorporeal removal — n (moderate to low dose 4 to 30 m. L/kg) : hemoperfusion within 12 hours of poisoning may reduce mortality > hemodialysis. -- up to two to three weeks after an ingestion n charcoal hemoperfusion more rapid reduction in plasma concentrations. n a new zeolite resin tested in vitro shows promise of a high degree of adsorption, although it has not yet been used clinically n 血液灌注應儘快於巴拉刈中毒 12小時內執行,黃金時間為食入 6 小時內。必須24小時內做血液灌注才有臨床意義,超過24小時則 因巴拉刈皆已被肺、肌肉等組織所吸收及累積,此時移除血液中 少量緩慢釋出的巴拉刈分子效果相當有限。
Ancillary treatment — n Immunosuppression — use of cyclophosphamide combined with corticosteroids: n Nitric oxide (not an established therapy, case report) — addition of nitric oxide (NO 25 ppm) to inspired gases→ transient improvement in arterial oxygenation in a single case report. In this, n Deferoxamine —Complexes with trivalent ions (ferric ions) to form ferrioxamine, which are removed by the kidneys n Pulmonary transplantation —without success
SUMMARY AND RECOMMENDATIONS — n ingested greater than 4 m. L/kg of paraquat concentrate administration of intestinal decontaminants + daily four to six hour hemoperfusion (or high efficiency hemodialysis) sessions. Daily hemoperfusion or hemodialysis treatment × 2~3 weeks. until paraquat is no longer detectable in blood. n Low-inspired oxygen therapy should be given until it becomes impractical in the face of hypoxemia. n The administration of steroids and cyclophosphamide may be considered. n More unconventional therapy with deferoxamine and nitric oxide inhalation may also prove useful.