Medicines from Cradle to Grave Session 1 Improving



 •")

































- Slides: 43
Medicines from Cradle to Grave Session 1 Improving Medicine Safety through Culture change Dr Liliana Risi
The day would be meaningful to me if… ‘I could understand more about the medicines I am issuing and more about script management and how to reduce wasteful repeats’- Prescribing Administrator ‘If I was sharing more with other Prescribing leads how to make prescribing safer and how we can learn from Medicine Errors’ - GP Prescribing Lead [only in contact with one other Prescribing Lead] ‘There was more primary and secondary sharing of learning as medicines are a big part of our job and in every consultation’ - Salaried GP ‘I came away understanding more about the system of prescribing that surrounds me as I feel anxious a lot as a Locum’ - GP Locum ‘If I felt that I had met others doing a similar job to me and how they were working with GPs’ - GP Pharmacist
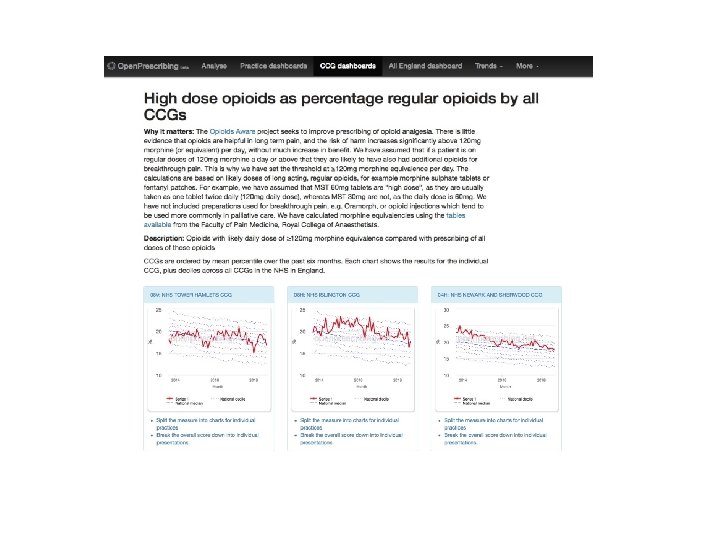
WIFI code 4 minutes • Who is who? Meet someone new • Patients! • 7 C’s - Celebrate, Courage, Connect, Curiosity, Collaborate, Consider, Compromise • TACA ‘talk about what you care about • Open Prescribing https: //openprescribing. net • Sign up to Safety https: //www. signuptosafety. org. uk
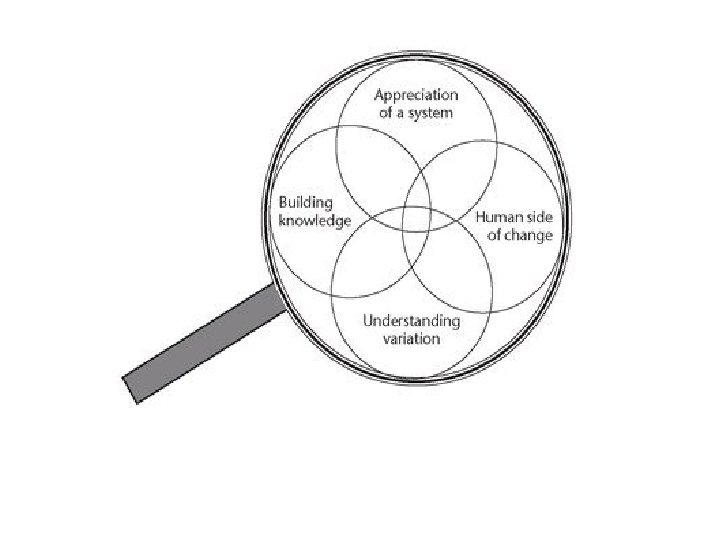
Tower Hamlets Appreciation of the system • Consultation rates are higher (social disadvantage) • >1, 500, 000 patient contacts/year (312 000 residents x average five contacts with GP/year) • 5 020 384 prescriptions issued 2017 -18 (150 -200/day in St Stephen’s HC) • NHS Cultural approach to error still characterised by blame
Human side of Medicines Roles • • GPs > 300 PN >100 Practice Pharmacists Prescribing Leads +/-36 GP Care Group Pharmacists >16 Prescribing Administrators ? Other – CHS?
Measuring and Understanding Variation Patient Experience Practice Population Primary Care Development Committee Diagnostics Activity Appointment Activity Medicines Activity Edenbridge - Real Time Integrated Data
Building Knowledge Medication Errors
Building Knowledge Medication Errors 237 million/Year occur at some point in the medication process (England) 66 million/year potentially clinically significant errors 71. 0% primary care (most medicines in the NHS are prescribed and dispensed) Errors more likely Older people Presence of co-morbidity Polypharmacy Adverse Drug Reactions (ADR) Primary care - hospital admission Secondary care - longer hospital stay NHS costs of definitely avoidable ADRs £ 98. 5 million/year 181, 626 bed days Tower Hamlets? Serious Incidents - high threshold (CCG), very few recorded How do we learn from patients: PPG, SEA, Complaints? PPG involvement? From each other in networks, localities? Serious Incidents –SEA/COMPLAINTS – learning isolated in practices Other CEG PROMIS (sulphonylurea, nsaid) EQUIP
25/5/18 A nine month old child is admitted with a 'diuretic overdose’ and discharged with 'no adverse effects noted from furosemide'
Having Safety Conversations using Appreciative Inquiry
Appreciative Inquiry Mindset 'diuretic overdose’ and discharged with 'no adverse effects noted from furosemide' Inquire into what works Commit to what it will be and identify first steps to bring you closer POSITIVE CORE Engage the team and agree how good it could be Imagine how good it could be
Appreciative Inquiry Conversations : How did this happen again? Practice Pharmacist Practice Prescribing Lead CCG Prescribing Advisor Practice GP CCG Medicines Optimisation Lead Mother CCG GP Lead for Children Community Pharmacist Barts Medicines Safety Barts Lead Pharmacist Paediatrics
Safer systems – ‘Handoffs’ • Learning as much as possible about the details of how people work • Intelligent Management of – Interface – Workforce – Working patterns: Part-time • Building Relationships marks the difference between safe and unsafe care • Embedding a restorative just culture instead of blame
Safety Cultures and Intrinsic Motivation
Simple Conversations
Building Knowledge: Restoring Hope! Intrinsic motivation and bottom up generation of metrics https: //www. lifeqisystem. com
Avedis Donabedian ‘Systems…are enabling mechanisms only. It is the ethical dimension of individuals that is essential to a system's success…the secret of quality is love. You have to love your patient, you have to love your profession’
Table Conversation Have a conversation with the person next to you about a recent error at your practice Use the appreciative enquiry approach of curiosity to identify moments in the process where something went well http: //www. evaluationsupportscotland. org. uk/s titch-time-working-groups/
Plenary What was your conversation about? How did you feel having the conversation?
https: //www. youtube. com/watch? v=Fq. Q-Ju. RDkl 8
Medicines from Cradle to Grave Session 2 Reducing Medicine Waste through Shared Decisions Dr Liliana Risi
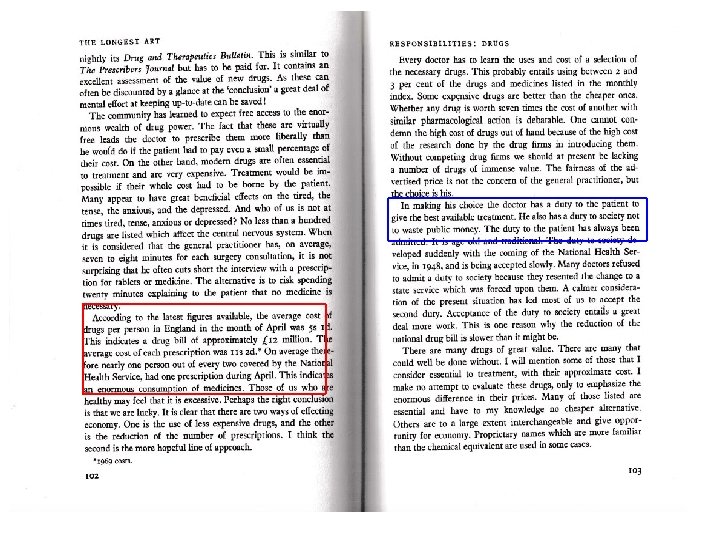
Medicine Costs • £ 17. 4 Billion in 2016/17 England hospitals account for nearly half of total NHS spending on medicines • £ 29. 5 Million 2017/2018 Tower Hamlets CCG
Medicine Prescribing Waste – what we do August 2018
Medicine Prescribing Waste – what we do
Patient’s experiences of chronic non-malignant musculoskeletal pain: a qualitative systematic review BJGP 2013 SPARROW
Waste – what happens? • Unused medicines cost the NHS approx £ 300 million every year – £ 110 million worth of medicine returned to pharmacies – £ 90 million worth of unused prescriptions being stored in homes – £ 50 million worth of medicines disposed of by Care Homes • Environment – 73 million inhalers are used in the UK every year and over 63% are placed in domestic waste bins after use, most ending up in landfill and the sea – *recycling of inhalers
The Effects of the Pharmaceutical Industry on the Ocean http: //oceancrusaders. org/pharmaceutical-ocean/
How do we waste medicines?
What do we do? We manage uncertainty Realising the full potential of primary care: uniting the ‘two faces’ of generalism. BJGP 2017 Joanne Reeve and Richard Byng 35
How do we manage uncertainty? C O N S E N T
Consent • • https: //handyapproachtocare. com Health literacy is the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions People with low health literacy may feel ashamed and try to conceal it from professional carers and family members People with long-term conditions reportmore difficulties in understanding health information and engaging with healthcare providers. Doctor’s health illiteracy A ‘culture of more’ is not necessarily better. Taking consent when professionals are burdened in areas characterised by poverty and inequality Consent to treatment A person must give permission before they receive any type of medical treatment, test or examination Mental Capacity Act and Medication Reviews Two questions may accomplish the major goals of advanced support preparation. 1. “If you cannot, or choose not to participate in health care decisions, with whom should we speak? ” 2. “If you cannot, or choose not to participate in decision making, what should we consider when making decisions about your care? ”
Concordance • If the person understands why they are taking a medicine they are more likely to take it • Language matters – Compliance ‘responding favourably to a request offered by others’ – Adherence ‘faithful attachment’ – Concordance ‘condition of agreement’
Shared Decisions- Value based Care • Ethical framework: Clinicians and patients work together to understand the patient’s situation and determine how best to address it • Shared Decision Making to Improve Care and Reduce Costs NEJM 2013 – 11 procedures yield more than $9 billion in savings nationally over 10 years – hip and knee replacements substantially reduced both surgery rates and costs — with up to 38% fewer surgeries and savings of 12 to 21% over 6 months • RCP 2016 & Cochrane Review Patient Decision Aids 2017 – are more satisfied with their care – are more likely to choose treatments based on their values and preferences rather than those of their clinician – tend to choose less invasive and costly treatments – improve their knowledge of the options – feel better informed and more clear about what matters most to them
Handy Approach to Care https: //handyapproachtocare. com Check list 5 Questions
e Br xit Vaccines Cancer drugs Insulin
Maya Angelou I've learned that people will forget what you said, people will forget what you did, but people will never forget how you made them feel
Bridge Over Diagnosis https: //www. youtube. com/watch? v=gfesu. NG 0 -k. Q