Malignant Tumors Primary Osseous Osteosarcoma Chondrosarcoma Nonosseous Ewings





 Serum alkaline phosphatase raised X-ray Radioisotope scan skip lesions")

















- Slides: 29
Malignant Tumors Primary Osseous : Osteosarcoma Chondrosarcoma Nonosseous : Ewing’s sarcoma Multiple Myeloma / Plasmacytoma Non-Hodgkin’s Lymphoma Metastatic bone disease
Osteosarcoma Primary osteosarcoma: unknown Secondary osteosarcoma: Paget's disease of bone, radiation injury, bone infarction Incidence: bimodal distribution Primary osteosarcoma: puberty/adolescence Secondary osteosarcoma: advanced age Sex: ♂ > ♀
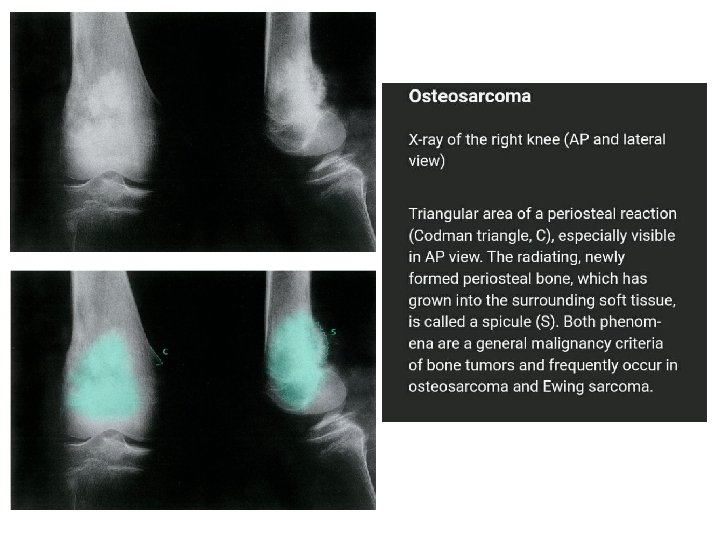
The sites most commonly involved are the metaphyseal region of long tubular bones, especially the region around knee joint 50% Pain is usually the first symptom; it is constant, worse at night and gradually increases in severity. Sometimes the patient presents with a lump. Pathological fracture is rare. Metastases
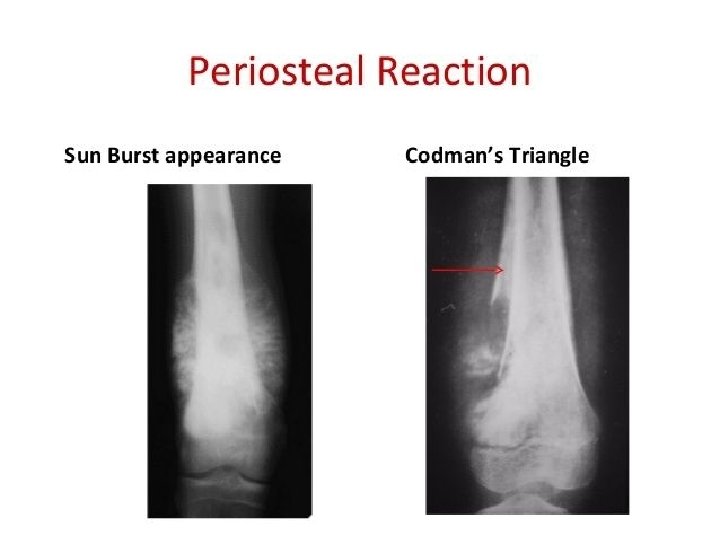
Investigations ESR ( raised ) Serum alkaline phosphatase raised X-ray Radioisotope scan skip lesions CT and MRI Chest X-ray done routinely Pulmonary CT ( to R/O metastatic dis. ) Biopsy Bone scan
Treatment 1. Chemotherapy 2. Surgery 3. Amputation
Prognosis • Depends mainly on the presence of metastasis at presentation • Osteosarcoma in Paget’s Dis. Is very aggressive (2 yrs survival is unusual with any type of surgery
• Chondrosarcoma • Arise from mesenchymal cells that produce cartilage • Location: Arises in the medulla of the long tubular bones, mostly in the lower limbs. The next most common sites are the pelvis , central skeleton and the ribs.
Occur either as primary tumor or a secondary change in a pre-existing benign chondroma or osteochondroma.
rings-and-arcs calcifications in the proximal humerus. The differential diagnosis is enchondroma or low grade chondrosarcoma. The CT shows the calcifications with subtle endosteal thinning of the cortical bone (arrows). Final diagnosis: low grade chondrosarcoma endosteal scalloping at the medial side which is a hallmark of chondrosarcoma.
Chondrosarcoma arising from osteochondroma Measuring the cartilage cap will help in distinguishing benign osteochondromas from chondrosarcomas. With 2 cm used as a cutoff for distinguishing benign osteochondromas from chondrosarcomas
Primary chondrosarcoma appears as a large lucent area encroaching upon or expanding the cortex. A characteristic feature is patchy calcification in the centre of the lesion, well demonstrated in this case. Note that the lateral cortex has fractured.
Treatment Complete surgical excision, as these tumor doesn’t respond to chemotherapy. Recurrence rate is high. Prognosis is related to grade of tumor (Low grade better prognosis) and the ability to completely surgically remove it
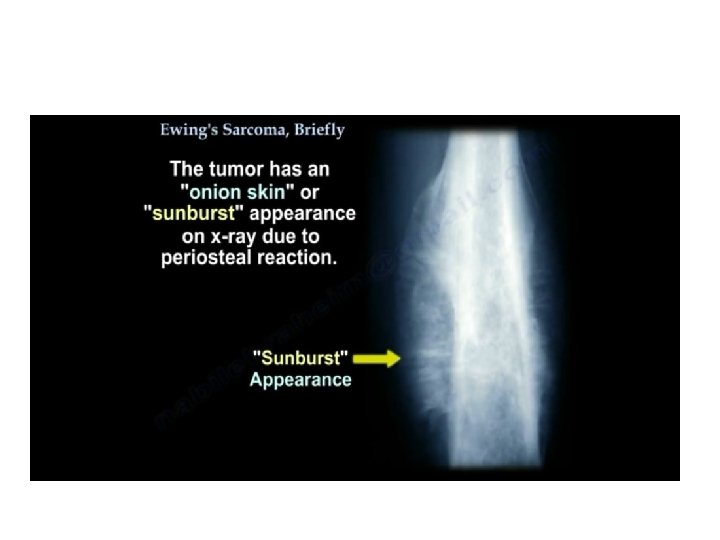
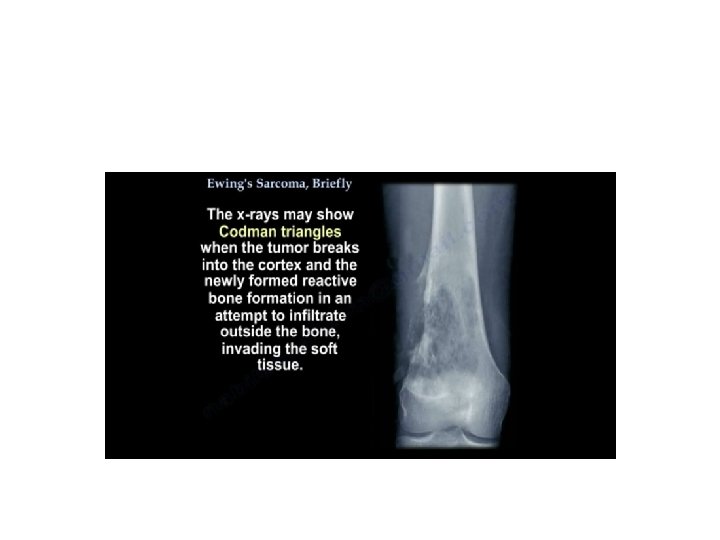
Ewing’s Sarcoma • Ewing’s sarcoma is believed to arise from endothelial cells in the bone marrow. • Incidence: peak at 10– 15 years. • Primary tumor: often diaphyses of long bones (particularly femur, tibia, fibula, and humerus) and bones of the pelvis. • Metastasis: lungs, skeletal system, bone marrow
• The patient presents with pain – often throbbing in character – and swelling. Generalized illness and pyrexia, together with a warm, tender swelling and a raised ESR, may suggest a diagnosis of osteomyelitis.
Diagnosis : Biopsy is Important Prognosis : The prognosis is always poor and surgery alone does llittle to improve it. Treatment : Chemotherapy, surgery then radiotherapy
Multiple Myeloma / Plasmacytoma - A malignant B-cell lymphoproliferative disorder of the bone marrow with plasma cell predominating. - Results in bone marrow cell proliferation and increased osteoclastic activity which lead to osteoporosis and lytic lesions throughout the skeleton (myelomatosis). - Plasmacytoma : is a large colony of plasma cells aggregates in one bone. Typical patient �� 45 -65 year old with weakness, bone pain backache with or without pathological Fracture. - Also, signs of hypercalcemia (thirst, polyuria and abdominal pain) plasma proteins abnormalities, increased blood viscosity and anemia -Late secondary features are due to renal dysfunction and spinal cord or root compression caused by vertebral collapse.
- X-ray : ü Multiple “punched out” defects in the skull, pelvis and proximal femur …’geographic map’ ü Crushed vertebra ü Osteocytes lesion in a large bone metaphysis Multiple myeloma is one of the commonest causes of osteoporosis and vertebral compression Fracture in men >45 y.
Investigations: Mild anemia High ESR Bence-jones proteins in urine Abnormal band in electrophoresis Increased creatinine and calcium Plasmacytosis with typical ‘myeloma’ cells in bone marrow puncture. Most common immunoglobulin in MM : Ig. G
D. D: - Other causes of bone loss - Metastasis bone disease - Paraprotineimia (gammopathies) - Always consult a hematologist Treatment : - Pain killer - Correct fluid disturbance and hypercalcemia - Immediate correction of spinal Fracture - Alkylating cytotoxic agents - Corticosteroids - Radiotherapy for solitary plasmacytoma. very useful