King Saud University College of Nursing Adult Nursing
 Fluid and Electrolyte Imbalance")
. Ø")



: − Contributing Factors: * Loss of water")


: − Contributing Factors: * Compromised regulatory")


: −Contributing Factors: * Use of a diuretic. *")

: − Contributing Factors: * Water deprivation in patient.")
")
: − Contributing factors: * Dirrhea, vomiting, gastric suctions.")



: − Contributing Factors: * Renal Failure. * Crush")




 Ca. Cl 10 cc of 10% solution")



. I- Isotonic")







- Slides: 38
King Saud University College of Nursing Adult Nursing (NUR 316) Fluid and Electrolyte Imbalance Acid and Base Imbalance 1
Introduction Ø Approx. 60% of the body weight is fluid (water and electrolytes). Ø Body fluid is located in 3 compartment: ü Intracellular fluids contained within the cells (ICF): 2/3 of TBF ü Extracellular fluid (ECF): 1/3 of TBF compose of IVF + 3 rd space (interstitial space which is the fluid between the cells ) ü Fluid compartment are separated by semi permeable membrane
DISTRIBUTION AND COMPOSITION OF BODY FLUID COMPARTMENTS 3 rd space IVF ICF
Average daily intake and output in an adult: Intake Oral Liquids 1300 ml. Water in foods 1000 ml. Water produced by metabolism 300 ml 2600 ml Output Urine 1500 ml Stool 200 ml Insensible lungs 300 ml Skin 600 ml 2600 ml
Normal Lab Results: - Na→ 135− 145 m. Eq/L. - K+ → 3. 5− 5. 5 m. Eq/L. - Ca++→ 8. 5− 10. 5 m. Eq/L. - Cl → 96− 106 m. Eq/L. - Mg→ 1. 5− 2. 5 m. Eq/L.
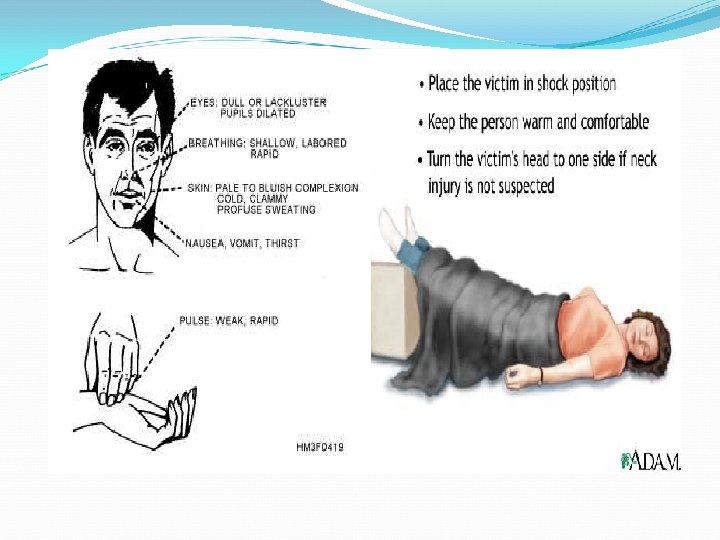
Fluid Volume Disturbance: I-Hypovolemia (fluids volume deficit): − Contributing Factors: * Loss of water and electrolyte. e. g. ( vomiting, diarrhea, burns). * Decrease intake. e. g. (anorexia, nausea, inability to gain access to fluids). * Some disease. e. g (D. M, Diabetic Insipidus). − Sings and symptoms: Weight loss, general weakness, dizziness, increase pulse.
Assessment & Diagnostic evaluation Health History & Physical examination Serum BUN & Creatinin Hematocrit level “great than normal” Urine specific gravity Serum electrolytes level Hypokalemia in case of GI & renal loss Hyperkalemia in case of adrenal insufficiency Hypernatremia insepedus in case of ↑insensible losses & diabetic
♣ Management treatment of the causes of FVD should be go with treatment of FVD itself factors influence the pt fluid needs should be taken in consideration In case of sever or acute FVD IV replacement should be started Isotonic solutions used to treat hypotension resulted from FVD Renal function & hemodynamic status should be evaluated ♣Nursing Management Monitor I&O as needed “urine” Monitor V/S, skin turgor , mental status & daily weight Extensive Hemodynamic CVP, arterial pressure Mouth care & ↓ irritating fluids
Fluid Volume Disturbance: II- Hypervolemia (fluid volume excess): − Contributing Factors: * Compromised regulatory mechanism such as renal failure, congestive heart failure, and cirrhosis. * Administration of Na+ containing fluids. * Prolong corticosteroid therapy. * Increase fluid intake. − Sings and Symptoms: Weight gain, increase blood pressure, edema, and shortness of breathing.
Assessment & Diagnostic Evaluation - Decreased BUN , Creatinin , Serum osmolality & hematocrete because of plasma dilution, &↓protein intake - Urine sodium is increased if kidneys excrete excess fluid - CXR may disclosed pulmonary congestion
Management ü Direct cause should be treated ü Symptomatic treatment consist of : v Diuretics v Restrict fluid & Na intake. v Maintained electrolytes balance v Hemodialysis in case of renal impairment v K+ supplement & specific nutrition Nursing Management: ü - Assess breathing , weight , degree of edema regularly ü - I & O measurement regularly ü - Semifowlers position in case of shortness of breath ü - Patient education
Electrolyte imbalance: I- Sodium. Deficit (Hyponatremia): −Contributing Factors: * Use of a diuretic. * Loss of GI fluids. * Gain of water. − Sings and Symptoms: Anorexia, nausea and vomiting, headache, lethargy, confusion, seizures.
Hyponatremia, continued Treatment: correct underlying disorder Fluid restrict, + diuretics Hypertonic saline to increase level 2 -3 m. Eq/L/hr and max rate 100 cc of 5% saline/hr
Electrolyte imbalance: II- Sodium Excess (Hypernatremia): − Contributing Factors: * Water deprivation in patient. * Hypertonic tube feeding. * Diabetes Insipidus. − Sings and Symptoms: Thirst, hallucination, lethargy, restless, pulmonary edema.
Hypernatremia, continued Treatment: correct underlying disorder Free water replacement: (0. 6 * kg BW) * ((Na/140) – 1). Slow infusion of D 5 W give ½ over first 8 hrs then rest over next 16 -24 hrs to avoid cerebral edema.
Electrolyte imbalance: III- Potassium Deficit (Hypokalemia): − Contributing factors: * Dirrhea, vomiting, gastric suctions. * Corticosteroid administration. * Diuretics. − Sings and symptoms: Fatigue, anorexia, nausea, vomiting, muscle weakness, change in ECG.
Hypokalemia, continued ECG changes in hypokalemia
Hypokalemia, continued ECG changes in hypokalemia
Hypokalemia, continued Treatment: Check renal function Treat alkalosis, decrease sodium intake PO with 20 -40 m. Eq doses IV: peripheral 7. 5 m. Eq/hr, central 20 m. Eq/hr and increase K+ in maintenance fluids.
Electrolyte imbalance: IV- Potassium Excess (Hyperkalemia): − Contributing Factors: * Renal Failure. * Crush injury, burns. * Blood transfusion. * Administration of IV K+. − Sings and Symptoms: Bradycardia, dysarrythmia, anxiety, irritable. - ECG: peaked T waves then flat P waves, depressed ST segment, widened QRS progressing to sine wave and V fib.
Hyperkalemia – ECG Changes
Hyperkalemia – ECG Changes
Hyperkalemia, continued Treatment: Remove iatrogenic causes Acute: if > 7. 5 m. Eq/L or EKG changes Ca-gluconate – 1 gm over 2 min IV Sodium bicarbonate – 1 amp, may repeat in 15 min D 50 W (1 ampule = 50 gm) and 10 U regular insulin Emergent dialysis Hydration and diuresis, kayexalate 20 -50 g, in 100 -200 cc of 20% sorbitol q 4 hrs or enema
Calcium Hypocalcemia: Seen in hypoalbuminemia. Check ionized Ca Often symptomatic below 8 m. Eq/d. L Check PTH: low may be Mg deficiency High think pancreatitis, hyper. PO 4, low Vitamin D, pseudohypoparathyroidism, massive blood transfusion, drugs (e. g. gentamicin) renal insufficiency S/Sx: numbness, tingling, circumoral paresthesia, cramps tetany, increased DTR’s, Chvostek’s sign, Trousseau’s sign EKG has prolonged QT interval
Calcium, continued Hypocalcemia cont. Treatment: Acute: (IV) Ca. Cl 10 cc of 10% solution = 6. 5 mmole Ca or Ca. Gluconate 10 cc of 10% solution = 2. 2 mmole Ca Chronic: (PO) 0. 5 -1. 25 gm Ca. CO 3 = 200 -500 mg Ca. Phosphate binding antacids improve GI absorption of Ca Vit D (calciferol) must have normal serum PO 4. Start 50, 000 – 200, 000 units/day
Calcium, continued
Calcium, continued Hypercalcemia Usually secondary to hyperparathyroidism or malignancy. Other causes are thiazides, milk-alkali syndrome, granulomatous disease, acute adrenal insufficiency Acute crisis is serum Ca> 12 mg/d. L. Critical at 16 -20 mg/d. L S/Sx: N/V, anorexia, abdominal pain, confusion, lethargy MS changes= “Bones, stone, abdominal groans and psychic overtones. ”
Calcium, continued Treatment: Hydration with NS then loop diuretic. Steroids for lymphoma, multiple myeloma, adrenal insufficiency, bone mets, Vit D intoxication. May need Hemodialysis. Mithramycin for malignancy induced hyper. Ca refractory to other treatment. Give 15 -25 mcg/kg IVP Calcitonin in malignant PTH syndromes
Types of IV solutions: * Serum plasma osmalarity (280 -300 m osmol). I- Isotonic Solutions: A solution with the same osmalality as serum and other body Fluids. e. g. N/S 0. 9%, Ringer Lactate, D 5 W. II- Hypotonic Solutions: A solution with an osmolality lower than that of serum plasma. e. g. half strength saline (0. 45% sodium chloride). III- Hypertonic Solution: A solution with an osmalality higher than that of serum. e. g. 1. 4 % NS
Hypertonic fluids Ø IVF have a higher osmolarity than the ICF &3 rd space. Ø Pulls fluid and electrolytes from the ICF &3 rd into IVF. 3 space H 2 O+ Elect rd H 2 O+ Elect
Hypertonic fluids Ø Can help stabilize blood pressure, increase urine output, and reduce edema. Ø Dangerous in the setting of cell dehydration. Ø Examples: 1. 4 % NS, Colloids & blood products
Hypotonic fluids ØIVF have a lower osmolarity than the ICF &3 rd space. Ø Pulls fluid and electrolytes from the IVF into the ICF &3 rd. H 2 O+ Elect 3 rd space
Hypotonic fluids ØCan be helpful when cells are dehydrated, hyperglycemic, diabetic ketoacidosis. ØCan cause cardiovascular collapse and increased Intracranial pressure (ICP) in some patients. ØExample: O. 45% Nacl, D 5 NS. 45 (5% dextrose in 1/2 normal saline).
Isotonic fluids ØIVF have same osmolarity as the ICF &3 rd space. ØFluid stay inside the IVF. H 20+ Elect 3 rd space
Isotonic fluids Ø After a few hours 80 % goes into 3 rd space while 20% stay in IV ( we need 3 liters of isotonic fluid to replace 1 liter of blood loss). Ø Can be helpful in hypotensive or hypovolemic patients. Ø Examples: Lactated Ringer's (LR), 0. 9% NS.
Question? 38