Jrome de Sze Jade Ghosn Franois Raffi Jeudi





 Stage II (Pulmonary phase) Severity of illness IIA Stage")
 Stage II (Pulmonary phase) Severity of illness IIA Stage")
 Stage II (Pulmonary phase) Severity of illness IIA Stage")


")
















 infection in patients")

 Death Hospitalized, on invasive mechanical ventilation or")

 Multivariate logistic regression,")



- Slides: 38
Jérome de Sèze | Jade Ghosn | François Raffi Jeudi 18 juin 2020 à 17 h 00
• Cette présentation a été réalisée en totale indépendance éditoriale par l’équipe de rédaction • Nous remercions le laboratoire Gilead pour son soutien institutionnel • Merci de répondre à quelquestions pour évaluer votre satisfaction à la fin de cette webconférence
Liens d’intérêts • Jérome de Sèze : Alexion, Biogen, Chugaï, CSL Behring, Genzyme, Novartis, Teva et Roche • Jade Ghosn : Gilead Sciences, Janssen, Merck et Vii. V Healthcare • François Raffi : Correvio, Gilead, Janssen, Merck, MSD, Pfizer et Vii. V Healthcare
1 Incubation Period Fever Cough Fatigue Anorexia Myalgias Diarrhea Critical illness in 5% of symptomatic patients Severe illness in 14% of symptomatic patients Dyspnea in 40 % of symptomatic patients -5 -4 -3 -2 -1 Median days from infection to onset of symptoms 1 2 3 4 5 6 7 8 9 10 11 12 Median days to onset after development of initial symptoms Onset of symptoms 13 14
2 Stage I (Early infection) Stage II (Pulmonary phase) Severity of illness IIA Stage III (Hyperinflammation phase) IIB Viral response phase Host inflammatory response phase Time course Clinical symptoms Mild constitutional symptoms Fever > 99, 6° F Dry cough, diarrhea, headache Shortness of breath Hypoxia (Pa. O 2/Fi. O 2 < 300 mm. Hg ARDS SIRS/Shock Cardiac failure Clinical signs Lymphopenia, increased prothrombin time, increased DDimer and LDH (mild) Abnormal chest imaging Transaminitis Low-normal procalcitonin Elevated inflammatory markers (CRP, LDH, IL-6, D-dimer, ferritin) Troponin, NT-pro. BNP elevation
3 Stage I (Early infection) Stage II (Pulmonary phase) Severity of illness IIA Stage III (Hyperinflammation phase) IIB ANTIVIRALS Viral response phase Host. ANTI-INFLAMMATORY DRUGS inflammatory response phase (IL-6 i, IL-1 i, JAKi…. ) Time course Clinical symptoms Mild constitutional symptoms Fever > 99, 6° F Dry cough, diarrhea, headache Shortness of breath Hypoxia (Pa. O 2/Fi. O 2 < 300 mm. Hg ARDS SIRS/Shock Cardiac failure Clinical signs Lymphopenia, increased prothrombin time, increased DDimer and LDH (mild) Abnormal chest imaging Transaminitis Low-normal procalcitonin Elevated inflammatory markers (CRP, LDH, IL-6, D-dimer, ferritin) Troponin, NT-pro. BNP elevation
3 Stage I (Early infection) Stage II (Pulmonary phase) Severity of illness IIA Stage III (Hyperinflammation phase) IIB ANTIVIRALS Viral response phase STEROIDS Host. ANTI-INFLAMMATORY DRUGS inflammatory response phase (IL-6 i, IL-1 i, JAKi…. ) Heparin Time course Clinical symptoms Mild constitutional symptoms Fever > 99, 6° F Dry cough, diarrhea, headache Shortness of breath Hypoxia (Pa. O 2/Fi. O 2 < 300 mm. Hg ARDS SIRS/Shock Cardiac failure Clinical signs Lymphopenia, increased prothrombin time, increased DDimer and LDH (mild) Abnormal chest imaging Transaminitis Low-normal procalcitonin Elevated inflammatory markers (CRP, LDH, IL-6, D-dimer, ferritin) Troponin, NT-pro. BNP elevation
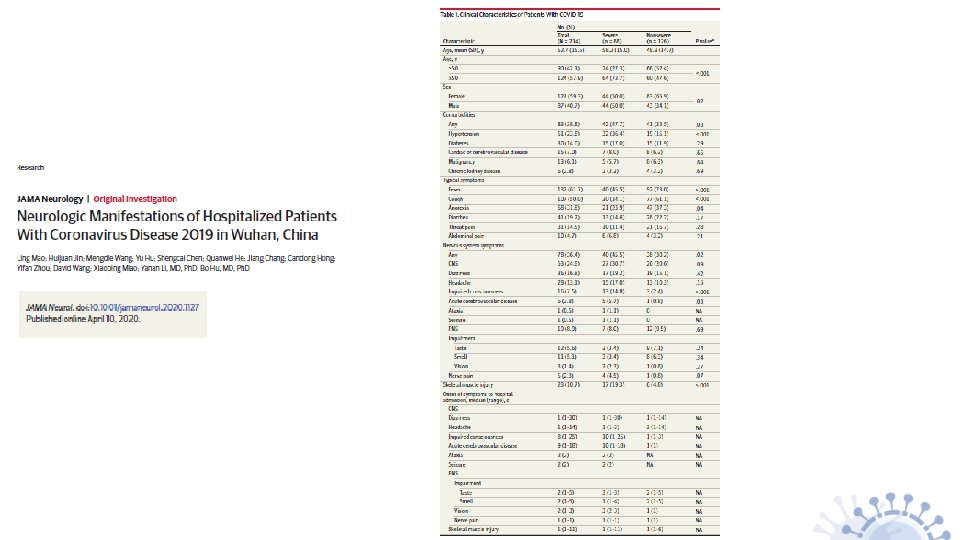
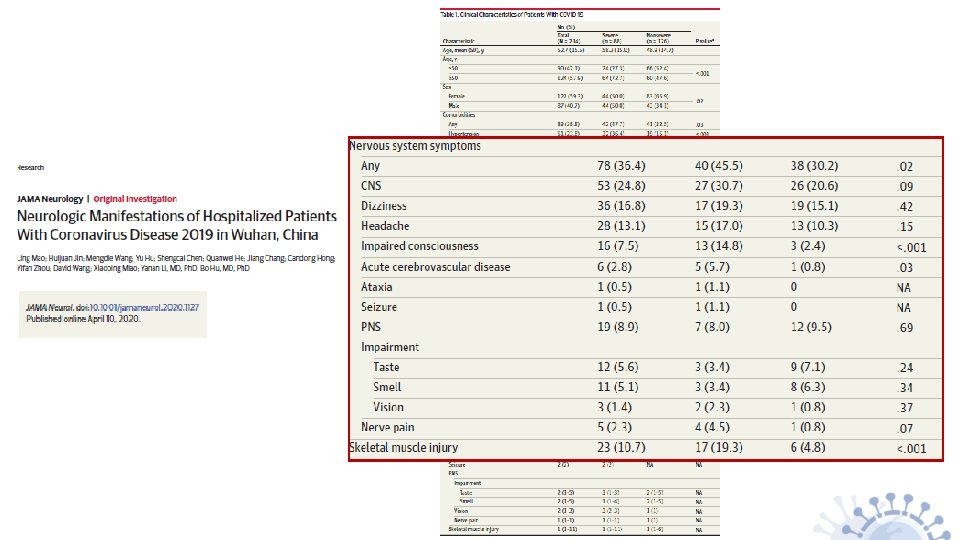
Complications neurologiques liées au COVID-19
COVID 19 : Complications neurologiques • Périphériques : SGB, Miller-Fischer
COVID 19 : Complications neurologiques • Centrales : Myélites, ADEM, Thrombophlébites, AVC (ischémiques/hémorragiques)
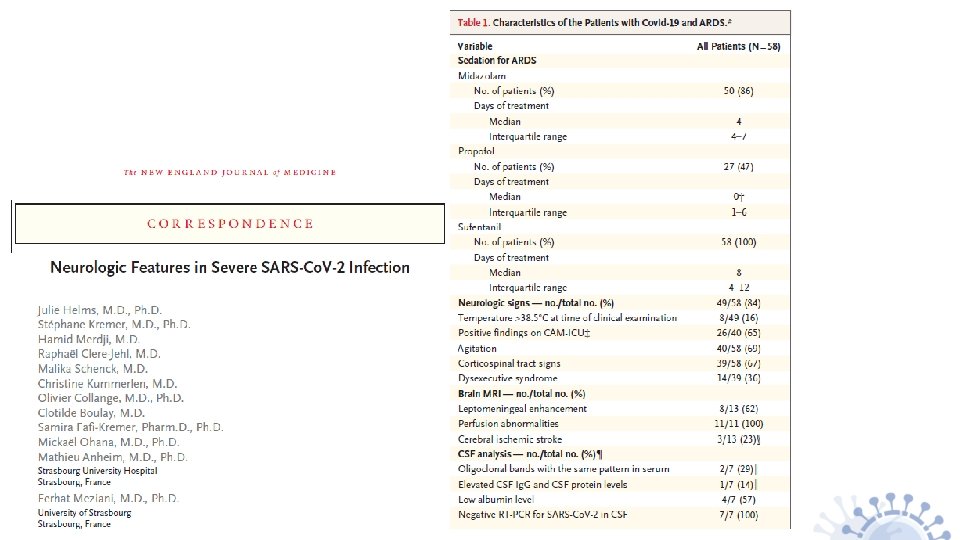
Aspects neuro-radiologiques
Table 1: Epidemiologic profile and clinical characteristics Kremer S et al. Radiology, in press
Table 2: Laboratory findings Kremer S et al. Radiology, in press
Table 3: Cerebrospinal fluid analysis Kremer S et al. Radiology, in press
Kremer S et al. Radiology, in press
Kremer S et al. Radiology, in press
Kremer S et al. Radiology, in press
Kremer S et al. Radiology, in press
COVID-19 : plus fréquent en cas d’immunosuppression/immunodépression ? Exemple de l’infection par le VIH
COVID-19 et VIH Baseline Characteristics of Patients Hospitalized With COVID-19 • Peu de cas rapportés dans la littérature • Un cas rapporté chez un PVVIH de 50 ans et greffé rénal (Kumar, Transpl Infect Dis 2020) • Plusieurs cas isolés rapportés : – en Ouganda (CD 4 > 900/mm 3, ARN-VIH < 1000 cp/ml) – Chypre (bon contrôle immunovirologique) – Iran – Singapour – Chine, Wuhan (1 patient avec CD 4 < 200/mm 3) – Turquie (4 patients, bien contrôlés) – New York (4 cas ambulatoires, tous bien contrôlés) Richardson, JAMA 2020 No. (%) Demographic information Total No. Age, median (IQR) [range], y No. (%) Comorbidities 5700 63 (52 -75) [0 -107] Sex Female Male 2263 (39. 7) 3437 (60. 3) Race No. African American Asian White Other/multiracial 5441 1230 (22. 6) 473 (8. 7) 2164 (39. 8) 1574 (28. 9) Ethnicity No. Hispanic Non-Hispanic Preferred language non-English 5341 1230 (23) 4111 (77) 1054 (18. 5) Insurance Commercial Medicaid Medicare Self-pay Other 1885 (33. 1) 1210 (21. 2) 2415 (42. 4) 95 (1. 7) Total No. Cancer Cardiovascular disease Hypertension Coronary artery disease Congestive heart failure Chronic respiratory disease Asthma Chronic obstructive pulmonary disease Obstructive sleep apnea 5700 320 (6) 3026 (56. 6) 595 (11. 1) 371 (6, 9) 479 (9) 287 (5. 4) 154 (2. 9) lmmunosuppression HIV History of solid organ transplant 43 (0, 8) 55 (1)
COVID-19 et VIH • 5 cas sur 543 patients hospitalisés pour COVID-19 à Barcelone (0, 98 %) Demographic and baseline HIV status Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Age (years) 40 49 29 40 31 Gender Transgender Male Transgender HIV-risk factor and exposure MSM, gym worker Bisexual man, health-care worker MSM, sexual worker participant in Chem. Sex session 6 day before MSM, dinner 5 days before with another person who was COVID-19 positive MSM, sexual worker Comorbidities None Hypothyroidism None Asthma None Year of HIV diagnosis 2007 2003 2013 2003 2020 Last CD 4 cell count (cells/µL) 616 445 604 1140 13 Last CD 4: CD 8 ratio 0, 8 0, 46 1, 1 1, 2 0, 1 HIV viral load at or before admission (copies/m. L) < 50 45 500 ART regimen before admission Tenofovir alafenamide, emtricitabine and darunavir -boosted cobicistat Abacavir, lamivudine and dolutegravir Tenofovir alafenamide, emtricitabine and darunavir -boosted cobicistat Abacavir, lamivudine and No ART: current diagnosis dolutegravir. Blanco, Lancet is late presenter HIV 2020 HIV status Blanco, Lancet HIV 2020
COVID-19 et VIH • • 33 PVVIH en Allemagne Tous sous c. ART 29/33 avec CD 4 > 350/mm 3 3/33 DDC • 45 PVVIH en Italie, 2 DCD (Gervasoni, CID 2020) Harter, Infection 2020 Age (y) Sex Years since HIV diagnosis Antir-retroviral treatment (ART) Years of ART CD 4/ CD 4 T-cell HIV-RNA T-cell CD 8 nadir (copies count ratio (count /m. L) 3 3 per mm ) 1 2 3 4 5 6 7 8 9 10 44 33 38 53 60 51 42 65 82 53 M F M M M M 14 7 3 11 7 20 17 13 28 10 DTG/ABC/3 TC RPV/TAF/FTC BIC/TAF/FTC NVP/ABC/3 TC DTG/TDF/FTC DTG/3 TC DTG/ABC/3 TC BIC/TAF/FTC DRV/RTV/RGV DRV/COBI/TAF/FTC 13 6 2 11 5, 5 10 5, 5 9 28 0, 5 754 619 1187 810 892 402 1087 1122 379 285 0, 83 0, 9 1, 52 0, 53 1, 00 0, 4 0, 93 0, 4 0, 25 163 387 541 293 362 329 439 490 151 204 < 50 < 50 920 842 11 12 13 14 32 31 37 37 M M M F 10 5 DRV/COBI/TAF/FTC EVG/COBI/TAF/FTC DOR/TDF/FTC 10 5 8 5 731 1000 946 402 1, 89 1, 15 1, 13 0, 5 325 810 580 NA < 50 15 36 M 4 DTG/ABC/3 TC 4 718 1, 2 NA < 50 16 68 M 14 DRV/COBI/TAF/FTC 14 499 0, 9 240 < 50 17 18 19 20 21 22 23 24 25 26 27 28 42 35 55 55 58 30 26 59 31 62 53 54 M M M 11 3 10 21 16 6 NA 15 7 20 6 15 RPV/TDF/FTC DTG/3 TC RPV/TAF/FTC BIC/TAF/FTC DTG/ABC/3 TC BIC/TAF/FTC DOR/TDF/FTC BIC/TAF/FTC NVP/TAF/FTC EVG/COBI/TAF/FTC BIC/TAF/FTC NA NA 10 21 14 6 NA 15 5 20 6 15 613 538 780 69 573 608 NA 718 647 692 717 437 1, 3 1, 0 1, 89 0, 06 0, 8 1, 00 NA 1, 75 1, 09 4, 94 0, 95 0, 68 430 419 370 8 314 608 NA 230 390 111 457 126 < 50 < 50 NA < 50 < 50 29 70 M 13 NVP/TAF/FTC 13 336 0, 38 250 < 50
Conclusions COVID-19 et VIH • Pas plus de COVID-19 chez les PVVIH • Formes pas plus sévère quand PVVIH infecté par COVID-19 • Facteurs de risque identifiés idem population générale
COVID-19 : plus fréquent en cas d’immunosuppression/immunodépression ? Exemple de la SEP
COVID et SEP : le registre COVISEP
Covi. SEP: Etude de cohorte évaluant les caractéristiques épidémiologiques de l’infection à Coronavirus (SARS-Co. V-2) chez les patients atteints de SEP ou de NMO • Cadre Il s’agit d’une étude épidémiologique observationnelle à visée descriptive et étiologique (hors loi Jardé) et vise à impliquer l’ensemble des neurologues hospitaliers et libéraux assurant le suivi des patients atteints de SEP et de NMO Objectifs 1. Caractériser la population de patients atteints de SEP ou de NMO infectés 2. Identifier les facteurs favorisant la survenue de forme sévère d’infection par le SARS-Co. V-2 chez les patients atteints de SEP ou de NMO Critères d’inclusion Patient atteint de SEP ou de NMO – Au moins un des quatre critères suivants : • COVID+ confirmés biologiquement • TDM thoracique typique • Anosmie ou agueusie d’apparition soudaine en l’absence de rhinite ou obstruction nasale • Symptômes typiques (triade associant toux, fièvre, asthénie) è Poursuite du recueil actuellement è Ajout dans le CRF des données de sérologies è Si question sur le recueil de la non-opposition : contact Yanica MATHIEU
Covi. SEP: cohort study to evaluate epidemiological characteristics Coronavirus (SARS-Co. V-2) infection in patients with MS os NMO-SD in France Diagnosis (n) MS (n=347) NMO (n=11) 44. 6 (12. 8) 249/ 98 13. 5 (10. 0) 6 CIS / 276 RRMS / 48 SPMS / 17 PPMS 2. 0 (0. 0 -9. 5) 35. 1 (11. 2) 9/2 7. 2 (6. 7) 1 AQP 4 / 2 MOG / 2 neg 3. 0 (0. 0 -6. 5) Demographics Age, mean (SD) Sex ratio (F/M) Disease duration, mean (SD) Disease course (n) EDSS, median (range) Comorbid conditions Cardiovascular disease Pulmonary disease Diabetes Obesity (BMI >30) Smoking 23 (6. 6%) 15 (4. 3%) 16 (4. 6%) 24 (6. 9%) 33 (9. 5%) 0 (0. 0%) 1 (9. 1%) 0 (0. 0%) 2 (18. 2%) 1 (9. 1%) 146/ 191 (76. 4%) 62/ 93 (66. 7%) 7/8 (87. 5%) 3/3 (100. 0%) COVID-19 diagnosis PCR COVID 19 positive, n/performed (%) Ground glass opacity on thoracic CT scan, n/performed (%) Louapre C et al. , JAMA Neurology, in press
Fréquence des symptômes 100 80 60 % 40 20 0 Louapre C et al. , JAMA Neurology, in press Asthénie Toux Fièvre Céphalées Gêne Respiratoire Anosmie Agueusie Troubles digestifs Vertiges
CMT (grouped according to systemic immunosuppression risk) Death Hospitalized, on invasive mechanical ventilation or ECMO Hospitalized, on non-invasive ventilation or high-flow oxygen devices 7 No risk 6 No treatment Interferon beta Glatiramer 5 Hospitalized, requiring supplemental oxygen 4 Hospitalized, not requiring supplemental oxygen 3 Not hospitalized, limitation on activities 2 Not hospitalized, no limitation on activities 1 Low risk Moderate/high risk Teriflunomide Dimethyl fumarate Natalizumab Other Fingolimod Ocrelizumab Rituximab Cladribine Alemtuzumab Clinical condition rating at NADIR and DMTs • • 0 73/347 patients have COVID-19 severity score ≥ 3 12/347 (3. 5 %) patients died from COVID-19 25 50 75 100 125 COVID-10 severity score 60 7 3 50 2 40 1 6 5 4 30 20 10 0 175 Number of patients 70 Number of patients 150 No treatment Interferon beta Glatiramer Louapre C et al. , JAMA Neurology, in press Teriflunomide Dimethyl fumarate Natalizumab Fingolimod Ocrelizumab Rituximab Cladribine Alemtuzumab Other
50 Number of patients 40 COVID-10 severity score 30 3 2 20 1 7 6 5 4 10 0 No treatment Interferon beta Glatiramer Teriflunomide Dimethyl fumarate Louapre C et al. , JAMA Neurology, in press Natalizumab Fingolimod Ocrelizumab Rituximab Ofatumumab Cladribine Alemtuzumab Other
Variables associated with severe COVID-19 (> hospitalization; clinical score > 3) Multivariate logistic regression, with stepwise variable selection Age (+10 yrs): 2, 49 (1, 92 -3, 22) Sex (Male): 2, 11 (1, 23 -3, 63) > 1 comorbidity : 2, 93 (1, 73 -4, 99) Cardiac comorbidity : 5, 72 (2, 39 -13, 66) Pulmonary comorbidity : 3, 53 (1, 23 -10, 07) Diabetes : 5, 36 (1, 93 -14, 95) Smoking : 0, 65 (0, 24 -1, 74) Obesity : 2, 95 (1, 25 -6, 94) Progressive course : 8, 22 (4, 52 -14, 96) EDSS < 3 : NA EDSS 3 - 5, 5 : 6, 28 (2, 97 -13, 26) EDSS ≥ 6 : 16, 10 (7, 72 -33, 58) No DMT : NA IFN/GA : 0, 07 (0, 02 -0, 25) TF/DMF/Nz/Other : 0, 18 (0, 09 -0, 36) Fg/Ocr/Rx/Clad/Alem : 0, 37 (0, 19 -0, 72) 10 -2 Age (+10 yrs): 1, 85 (1, 39 -2, 46) Sex (Male): 1, 61 (0, 83 -3, 11) Obesity: 2, 99 (1, 03 -8, 70) Cardiac comorbidity : 2, 68 (0, 97 -7, 40) EDSS < 3 : NA EDSS 3 - 5, 5 : 3, 48 (1, 55 -7, 84) EDSS > 6 : 6, 33 (2, 78 -14, 39) 10 -1 100 Lower risk 101 Higher risk 102 Odds ratio 10 -2 10 -1 100 Lower risk 101 Higher risk Odds ratio, 95% confidence interval Louapre C et al. , JAMA Neurology, in press 102 Odds ratio
8 EDSS 6 4 2 0 20 Louapre C et al. , JAMA Neurology, in press 30 40 50 Age 60 70 80
Conclusions COVID-19 et SEP • Peu de complications neurologiques dans la population COVID peu sévère • Complications grave dans les formes « réanimatoires » = nécessité d’une évaluation au long cours… • Pas plus de COVID-19 chez nos SEP y compris sous immunosuppresseurs • Formes pas plus sévère quand SEP infecté par COVID-19 • Facteurs de risque identifiés idem population générale
Jérome de Sèze | Jade Ghosn | François Raffi Jeudi 18 juin 2020 à 17 h 00