Epidural anesthesia and analgesia Anesthesiology dep R 2

, lumbar,")



























- Slides: 30
Epidural anesthesia and analgesia Anesthesiology dep. R 2 Mei-Hui, Yang 2004/08/16
Wide application l l l Epidural block can be performed at the sacral(caudal), lumbar, thoracic or cervical levels. Epidural techniques are widely used for operative anesthesia, obstetric analgesia, postoperative pain control, and chronic pain management. Dose judgment could be single shot, intermittent bolus or continuous infusion or combined.
l Differential block: By using relatively dilute concentrations of local anesthetic combined with an opiate, an epidural can block the smaller sympathetic and sensory fibers wile sparing the larger motor fibers.
l Segmental block: Due to local anesthetic is not spreadily in CSF as spinal anesthesia, a well-defined band of anesthesia at certain nerve roots without those above and below blocked can be achieved with epidural techniques.
Advantages in conjugation with GA l CV systems: Blockade of cardiac sympathetic innervation (arise at T 1 -T 4) with dilute local anesthetic postoperatively via a thoracic epidural catheter can reduce myocardial ischemia in patients with coronary artery disease.
Respiratory system l Thoracic or upper abdominal surgery is associated with 1. decreased diaphragmatic function postoperatively from decreased phrenic nerve activity 2. decreased FRC these can lead to atelectasis and hypoxia via V/Q mismatch
l Some evidence suggests that postoperative thoracic epidural analgesia in high-risk patients can improve pulmonary outcome by decreasing the incidence of pneumonia and respiratory failure, improving oxygenation, and decreasing the duration of mechanical ventilatory support
Metabolic and endocrine system l l Surgical trauma produces increases in ACTH, cortisol, epinephrine, norepinephrine and vasopressin and activate RAA system. Neuraxial blockade can partially suppress (during major invasive surgery) or totally block (during lower extremity surgery) this stress response and then reduce perioperative arrhythmias and the incidence ischemia possibly. A T 11 block can block adrenal pathways and blunt hyperglycemia.
Complication of neuraxial block l l l Backache Headache Urinary retention Maternal fever Transient neurologic symptoms (TNS): back pain radiating to the legs without sensory or motor deficits, occurring after the resolution of spinal block and resolving spontaneously within several days
l l l l High or total spinal anesthesia Subdural injection Cardiac arrest Systemic toxicity Cauda equina syndrome & other neurologic deficits, transient or permanent Maningitis & arachnoiditis Epidural abscess Spinal & Epidural hematoma
Paraplegia after delayed detection of inadvertent spinal cord injury during thoracic epidural catheterization in an anesthetized elderly patient Ming-Chang Kao, MD, Shen-Kou Tsai, MD, Ph. D, Mei-Yung Tsou, MD, Ph. D Dep. Of Anesthesiology and Radiology, TVGH Anesth Analg 2004, Aug. ; 99: 580 -3
Foreword l l Permanent paraplegia after epidural anesthesia is extremely rare; the incidence is <0. 02% The cause are diverse, including epidural hematoma, epidural abscess, direct cord trauma, spinal infarction and neurotoxicity by accidental subarachnoid injection or chemical contamination.
Case report l l l An 81 -yr-old man with acute cholecystitis and common bile duct stones underwent open cholecystectomy and choledocholithotomy. Medical hx: HTN with baseline BP 166/67 mm. Hg Thoracic epidural for postoperative pain relief was suggested
l l After explanation the possible risks, including potential cord injury, the procedure was performed after the induction of GA due to his fear about the procedure when he was awake. With left lateral position, a 17 -gauge Tuohy needle was introduced at the T 910 interspace.
l l l Three needle passes were made to locate the epidural space by using the loss-of-resistance-to-air technique. A 19 -gauge single-end port catheter was inserted 3. 5 cm cephalad. There was some resistance to catheterization through the needle. Catheter aspiration was negative.
l l Lidocaine 2% 2 ml with 1: 200000 epinephrine was injected as a test dose. The arterial BP slightly decreased from 130/64 to 110/52 mm. Hg 5 min later. Ten minutes after the test dose injection, an epidural bolus of 0. 2% bupivacaine 8 ml with morphine 1 mg was given. ABP gradually decreased to 70/40 mm. Hg within the next 10 min but returned to 110/60 mm. Hg after ephedrine 16 mg and lactated Ringer’s solution 500 ml IV were administered.
l l OP lasted for 2. 5 h and was uneventful. In the PACU, he was pain free and did not complain of motor or sensory impairment. PE showed freely movable extremities but relative weakness in the lower extremities, with muscle strength of 4/5 and poor response to pain and sensory stimulus.
l l Negative catheter aspiration was confirmed again to exclude intrathecal placement. PCA pump was then programmed to deliver 0. 1% bupivacaine with fentanyl 1 ug/ml at a basal rate of 4 ml/h, with a demand dose of 2 ml and a lockout interval of 20 min. The SBP was 100 -130 mm. Hg in the PACU and he was returned to the ward 1 h later without significant further decreases in muscle strength.
l l l The patient first complained of numbness and weakness of the lower extremities 8 h after surgery, early the next morning. NE revealed: 1. sensory loss below T 11 2. paraplegia with no movement of either lower extremity No blood was aspirated from the catheter and then the catheter was removed.
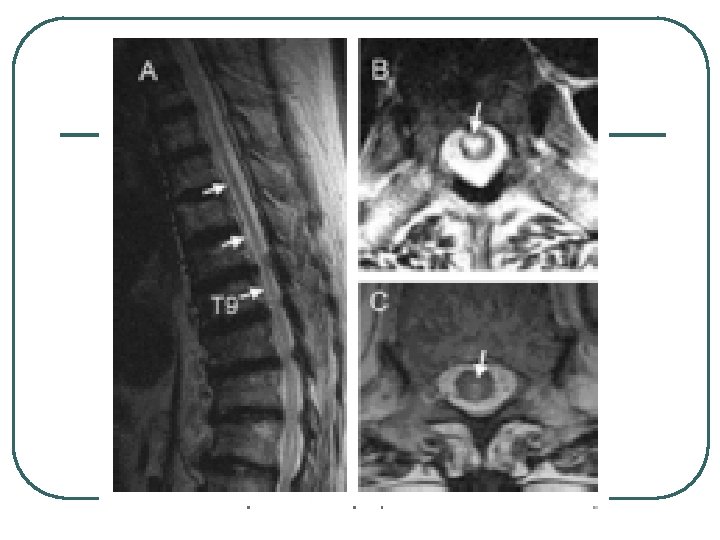
l l l A total volume of 44 ml of bupivacaine with opioid was given. NE remained unchanged 4 h after discontinuation of the pump infusion. Emergent CT showed an intramedullary 2. 4 -mm-diameter air bubble at T 9.
l l MRI revealed extensive intramedullary abnormally high signals on T 2 -weighted images from dorsal T 12 extending upward to ventral T 4. The intramedullary air bubble at T 9 was noted on MRI, too.
Following treatment l l Methylprednisolone 30 mg/kg IV bolus over 15 min, followed y a 5. 4 mg/kg/h IV infusion for the next 23 h was given according the neurologist’s suggestion. Summarized neurologic deficits on postoperative Day 3 revealed bowel and bladder incontinence, flaccid paraplegia with areflexia, loss of pain and temperature perception but preservation of touch and position sensations of both legs.
l l MRI on postoperative Day 22 revealed a small residual intramedullary abnormally high signal on T 2 W at ventral T 8 The final follow-up 6 mo later showed partially improved sensory function of the lower extremities and muscle strength to 1 -2/5.
Discussion l l Severely spondylotic spine The air injected into the spinal cord split the cord and thus facilitated the following catheterization The “some resistance” to catheterization was ignored The hypotension after the initial epidural bolus dose during surgery and the relative postoperative hypotension were attributed to the intramedullary bupivacaine and opioids.
l l The pump infusion may have increased the intracord pressure and compormised cord perfusion resulting in a vicious cycle of cord injury. In addition to the residual anesthetic effects, the intramedullary bupivacaine and opioids should have masked the patient’s discomfort during the continuing cord trauma.
l Besides, delayed response of this elderly patient and lack of regular neurologic checkups by acute pain team members at night also served as obstacles to early recognition.
l There was no direct neurologic complication related to lumbar epidural catheterizations in 4298 anesthetized patients. ~by Horlocker et al Anesth Analg 2003; 96: 1547 -52 l There are insufficient data to support the assumption of increased risks of thoracic epidural catheterization under general anesthesia.
l l Two thirds of the patients with neurologic deficits had either a paresthesia during needle placement or pain on injection. ~Yves Auroy, M. D, Anesthesiology, V 87, No 3, Sep 1997 As a result, thoracic epidurals was suggested to be performed only in conscious patients. This will not eliminate the risks of cord injuries but will help to identify them earlier.