The Evolution of the Epidural Needles Joseph Eldor



, Chromium (18%), Nickel (9%), Manganese (1. 5%),")









")












 needle")






")


")








, the Crawley needle (1968), the Foldes needle (1973)")

 with a pencil point design for single-shot")

, a Tuohy needle with a Luer lock hub.")







 through the dural hole made by the spinal needle")
 and catheter insertion (B) into the subarachnoid space in")








")


 was polyethylene. It was soon replaced by polyvinyl chloride because")






 and closed-end (three lateral holes)")













 of 39 patients Westbrook et al. found that the")





")
 has its")





- Slides: 112
The Evolution of the Epidural Needles Joseph Eldor, MD
All Epidural Needles Are Not Created Equal
Spectral analysis of epidural needles
Epidural needles are composed of Iron (69%), Chromium (18%), Nickel (9%), Manganese (1. 5%), Silicone(0. 5%) and Molybdenum (between 0. 2% to 2. 7%). Different needles – different compositions…
Hardness of the needles and stilletes
Epidural needles differ also by the hardness of the needles and stilletes.
For example, BD 18 G Tuohy needle is 383 VPN Vs. BD 18 G Crawford needle’s 507 VPN. Again, different needles – different composition…
Dimensions and clearance of needles
Epidural needles differ also by their dimensions. For example, the inner diameter of the BD 18 G Tuohy needle is 1. 053 mm while the Portex 18 G Tuohy needle’s is 1. 220 mm…
However, Epidural anesthesia is an integral part of today’s practice of Anesthesiology.
A change in needle design was significant among the improvements.
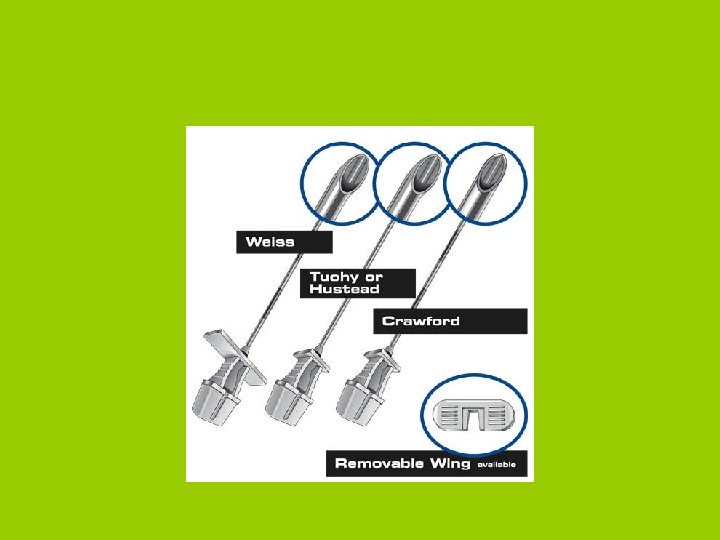
Epidural needles are often very broadly referred as “Tuohy needles” even though their needle tip configuration is much closer to that of a Hustead needle design.
In 1901 the French Radiologist Jean Anthanase Sicard described injecting dilute solutions of cocaine through the sacral hiatus to treat patients suffering from severe intractable pain or lumbago.
Dr. JEAN ANTHANASE SICARD (1872 -1929)
Fernand Cathelin reported similar work 3 weeks later than Sicard. He recognized that sacral injections of cocaine might also be used for surgery.
In 1921 a Spanish surgeon Fidel Pagés described a lumbar approach to epidural anesthesia.
In 1933 an Italian surgeon Archile Mario Dogliotti performed abdominal surgery with single shot lumbar epidural anesthesia.
Most medical historians date the regular use of epidural anesthesia from Dogliotti’s article: Dogliotti AM. A new method of block: segmental peridural spinal anesthesia. Am J Surg 1933; 20: 107 -18
However, a Romanian obstetrician , Eugene Aburel, injected chinocaine through a silk ureteral catheter to block the lumboaortic plexus of laboring women two years before Dogliotti, in 1931.
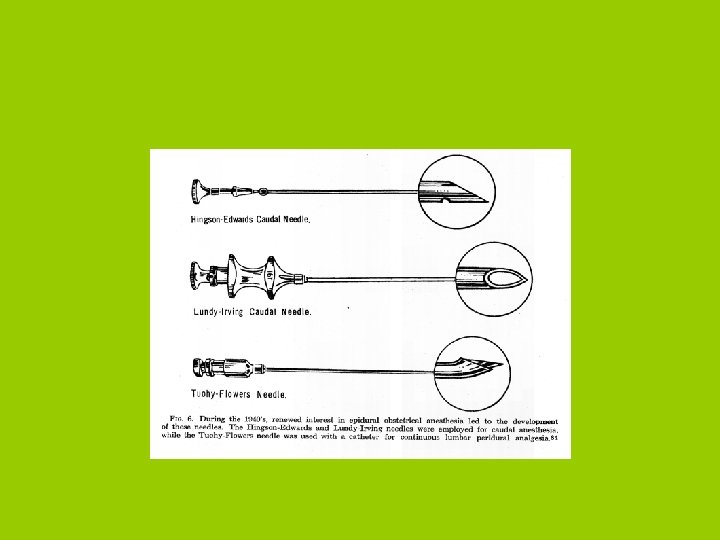
In the USA, Hingson and Edwards devised a method for continuous caudal anesthesia and used it on 33 laboring patients in 1942.
Two years later, in 1944, Hingson and Southworth described a lumbar approach for continuous epidural anesthesia using a 15 gauge Barker spinal needle and a silk ureteral catheter “to but not into the peridural space”. They obtained satisfactory anesthesia in only 10 of 16 patients.
BARKER NEEDLE
Ralph L. Huber designed in 1946 a needle with a directional tip which allowed anesthesiologists to direct the catheter as it exited the needle tip (US patent 2 409 979. October 22, 1946).
Although Huber intended this needle for IV and tissue injections, Edward B. Tuohy recognized that the directional point might facilitate placement of spinal catheters.
Tuohy also added a stylet, thereby hoping to further decrease the risk of skin plugging.
The Cuban anesthesiologist, Manuel Martinez Curbelo, described in 1949 the use of a 16 gauge Huber (Tuohy) needle with a 3. 5 F silk ureteral catheter for continuous segmental lumbar peridural anesthesia.
Charles E. Flowers, an obstetrician at Johns Hopkins University, altered the Huber (Tuohy) needle by blunting the bevel and designing the stylet to protrude past the needle tip in 1949.
However, Robert Hustead, another Hopkins colleague, called the Tuohy-Flowers modification a “technical nightmare”…
However, Flower’s idea of a blunt tip did have appeal, and it became part of further enhancements by Crawford, Weiss, Sprotte and even Hustead himself.
Robert Hustead made his own modifications to the Tuohy-Huber needle by hand by using a stone and a needle sharpener…
Hustead sanded off the sharp tip of the original Tuohy-Huber needle and changed the angle of the bevel. The result was a needle opening that did not exceed 2. 7 mm in length, with an angle of the needle bevel of 12º-15º.
(Robert F. Hustead (born: 1928
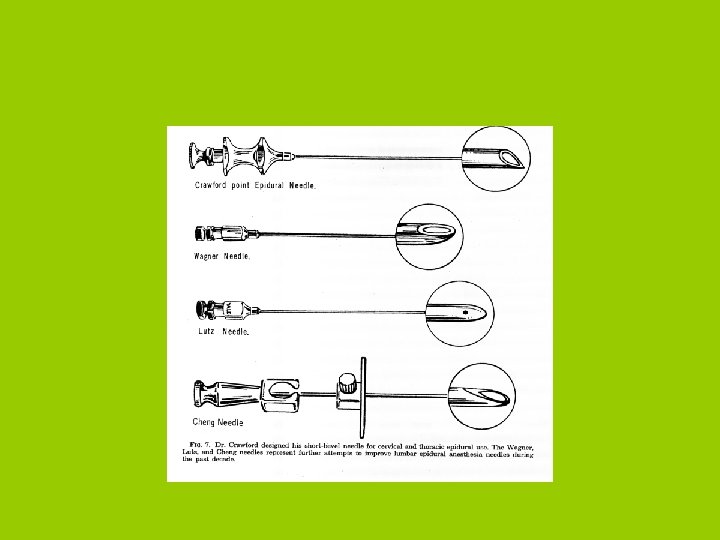
Crawford described in 1951 the use of an epidural needle with a straight tip in 677 patients for thoracic surgery. The Crawford epidural needle was a Quincke type with an extremely short, and thus a very blunt, bevel. The bevel of his needle was very flat (60º if measured from the longitudinal axis of the needle).
Oral Bascom Crawford (born: 1921)
CRAWFORD EPIDURAL NEEDLE
Jess Weiss dulled the needle tip and added “wings” to make it easier to grasp the needle with both hands for placement.
Jess Bernard Weiss (born: 1917)
WEISS TUOHY NEEDLE
Jürgen Sprotte of Würzburg, Germany developed in 1979 a pencil point needle for spinal anesthesia, similar to one designed by Hart and Whitacre but with a noticeable difference in its tip geometry: the original Whitacre needle had a short, cylindrical-tip configuration, whereas Sprotte used the olive-shaped, rounded-tip geometry.
In 1987 Sprotte started to experiment to make his needle more suitable for epidural use. He added a special plastic wedge to the inside of the needle tip that would direct an epidural catheter toward the lateral needle hole.
(Jürgen Sprotte (born: 1945
Epidural Sprotte Spezial Needle
Other Epidural Needles
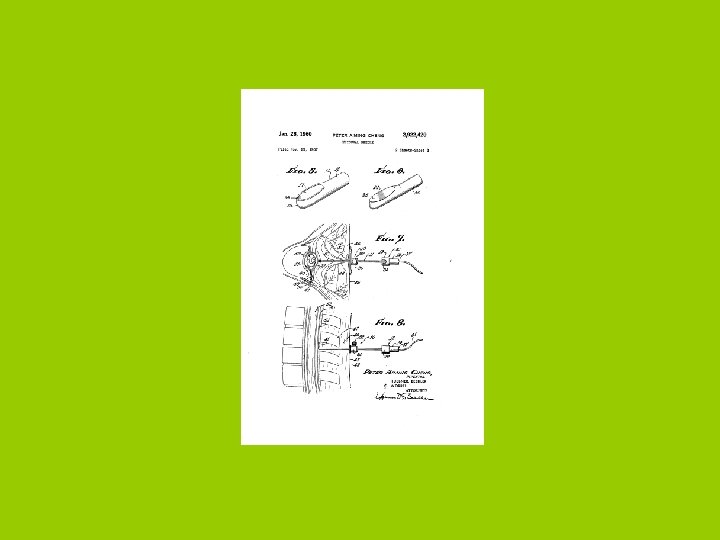
Cheng needle was described in 1957. It was the first epidural needle with centimeter markings to indicate depth (US patent no. 2 922 420).
Unfortunately, the Cheng needle was described as “cumbersome” to use and “extremely difficult to effect”.
There also the Wagner needle (1957), the Crawley needle (1968), the Foldes needle (1973) and the Bell needle (1975) – all variants of the Huber design with a blunted tip of varying sharpness.
There is the Brace needle, a Crawford variant.
There is the Lutz epidural needle (1963) with a pencil point design for single-shot epidural use.
Lutz epidural needle
There is the Scott needle (1985), a Tuohy needle with a Luer lock hub.
Aldrete 25 G Epidural Needle Pain Digest 8: 260 -263, 1998
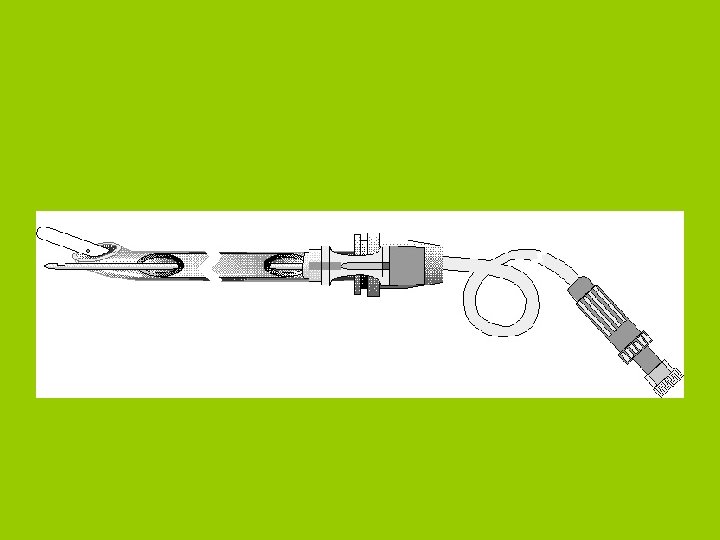
Eldor, Coombs and Torrieri Needle Eldor and Torrieri described in separate letters, in 1988, an epidural needle with a spinal needle attached to it. Through the spinal needle a longer spinal needle is inserted into the subarachnoid space, while an epidural catheter is introduced through the epidural needle into the epidural space. A few months before the publication of these letters, Coombs applied for a patent on the same device.
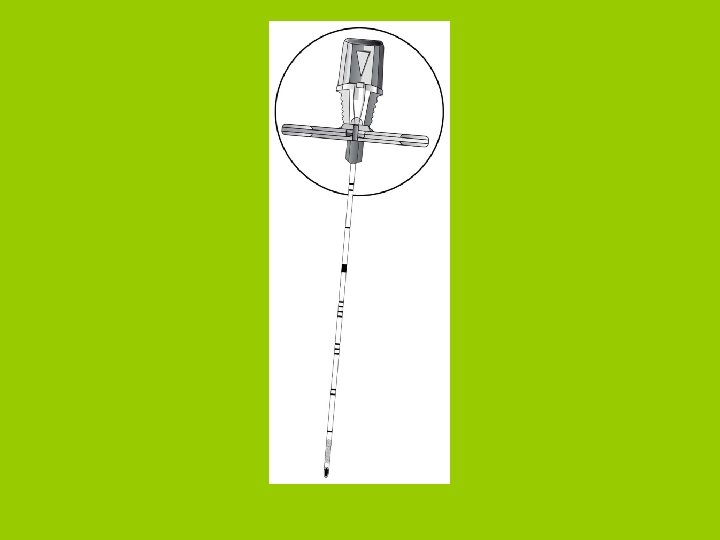
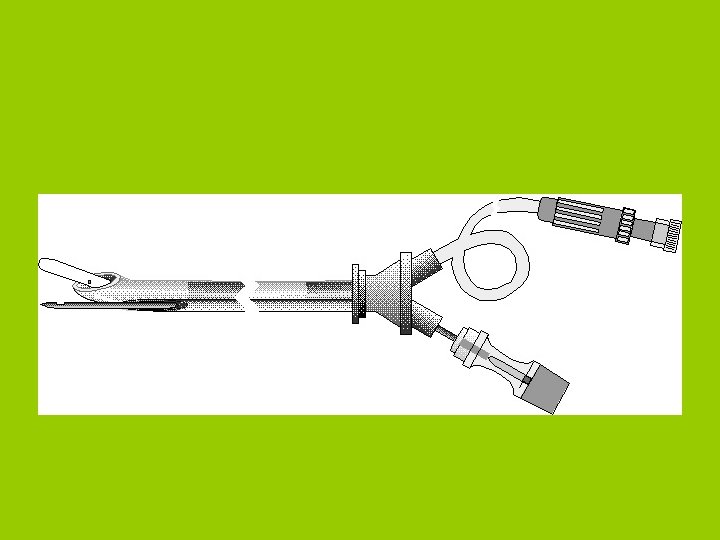
Eldor Needle The Eldor needle was first described in 1990. The Eldor needle is a combined spinalepidural needle which is composed of an 18 gauge epidural needle with a 20 gauge spinal conduit. This is a specialized needle for the combined spinal-epidural anesthesia.
The spinal conduit of the Eldor needle serves as a break at the ligamentum flavum for an inadvertent insertion into the spinal space
Eldor CSEA needle
Needle-through-needle technique Coates from England Mumtaz, Daz and Kuz from Sweden, in two separate letters in the same issue of Anaesthesia, in 1982, first described the insertion of a long spinal needle through the epidural needle for performing the combined spinal-epidural anesthesia. Coates found the technique "simple, reliable and relatively quick to perform". After injecting the anesthetic solution into the subarachnoid space, the spinal needle is withdrawn and an epidural catheter is threaded through the same lumen of the epidural needle, through which the spinal needle was inserted.
Metallic microparticles are produced by the friction between the two needles in the needle-through-needle technique
Inadvertent epidural catheter protrusion (B) through the dural hole made by the spinal needle (A) in the needle-through-needle technique
Inadvertent epidural needle protrusion (A) and catheter insertion (B) into the subarachnoid space in the needle-through-needle technique
A. Needle-through-needle technique: The Whitacre pencil point spinal needle deflects by 10 degrees from the tip of the epidural needle. B. Eldor needle technique: The double-hole pencil point spinal needle exits the spinal conduit of the Eldor needle in a straight direction and parallel to the epidural tip.
Huber needle technique Huber, the inventor of the "Tuohy" epidural needle, also patented in 1953 an hypodermic needle with an "auxiliary outlet being disposed in transverse alignment with the channel outlet". Hanaoka described in 1986 its use in 500 patients. This needle has a very small hole behind the epidural needle tip ("back eye"). A small gauge spinal needle is inserted through that hole and punctures the dura. After withdrawing the spinal needle an epidural catheter is introduced through the epidural needle.
Espocan Tuohy Needle
”The “Twin Theory
CSEA: "To paint the fence" from both its sides
The first technical advancement over the early years of epidural anesthesia was the downsizing of the catheter and needle combination used.
Tuohy’s idea of using a lacquered silk catheter for continuous spinal anesthesia was stimulated by his neurosurgical colleague, Dr. Love, who already used this catheter for subarachnoid drainage at the Mayo Clinic.
Whereas Love had advocated the use of a 5 F ureteral catheter in combination with a 13 gauge Barker needle, Tuohy used a 15 gauge Barker needle and a 4 F ureteral catheter in 1944.
Edward Boyce Tuohy (1908 -1959)
Some years later, in 1949, Curbelo advocated the use of a 3. 5 F silk catheter with a 16 gauge Tuohy needle.
The use of plastic catheters was first described by Flowers et al. in 1949.
The first polymer (plastic) was polyethylene. It was soon replaced by polyvinyl chloride because of its low melting point, which, similar to the lacquered silk catheter, made it prone to swelling and deformity with sterilization.
More recent polymers are nylon, Teflon, polyurethane and silicone.
Most of the epidural catheters used in the USA are of the single terminal hole, while most of those used in the UK are of the three lateral holes with a blunted end.
Curbelo in 1947 was the first to use an epidural catheter for epidural anesthesia. It was of the end hole type.
Lee in 1962 described an epidural catheter which its "tip is non-patent and smooth, to facilitate insertion, solution enters the space from a small opening 1 cm from the tip".
Skinner in 1966 described another epidural catheter with "the tip of the cannula. . . is blunt. . . and has a hole in its end. There is a second hole, 3 mm from the distal end". He said that "with the hole in this position, kinking is impossible with the stresses involved in normal use".
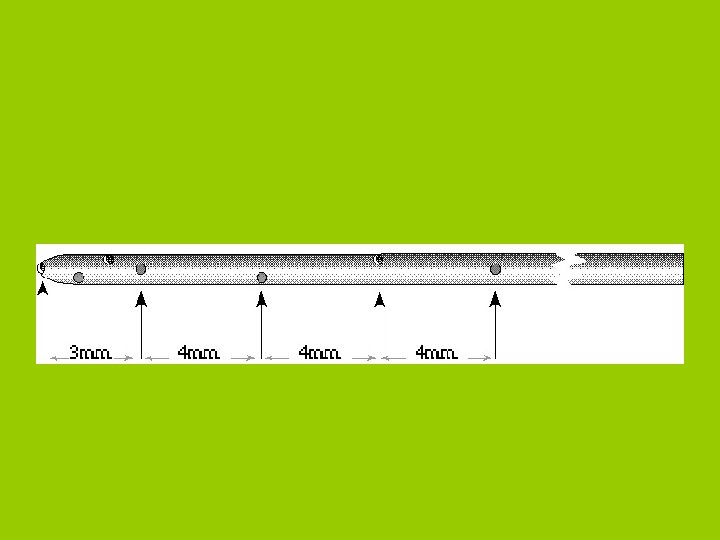
Collier and Gatt described in 1993 an epidural catheter, with a closed end and three holes spaced at approximately 2, 3 and 4 mm from the smooth closed tip. They suggested that the close spacings of the holes will eliminate the complication of multi-compartment block (epidural, spinal or intravenous), as seen with earlier multihole epidural catheters.
Michael et al. compared between the openend (single hole) and closed-end (three lateral holes) epidural catheters. They found that the open-end catheters "caused an unacceptably high incidence of unsatisfactory sensory blockade".
Collier and Gatt also found the incidence of unsatisfactory blocks with terminal hole catheter to be "unacceptably High" (32%) when compared with the three lateral holes catheter (12%).
Eldor described in 1998 the CEMLH epidural catheter that has 7 holes within its 1. 5 cm head: One at the tip while the 6 lateral holes are arranged circumferentially from each other (US patent no. 5 800 407).
Evaluation of epidural needles
Dural tissue trauma and cerebrospinal fluid leak after epidural needle puncture: effect of needle design, angle, and bevel orientation.
Cerebrospinal fluid leak after puncture was influenced most by epidural needle gauge. Leak rate was significantly less for the 20 gauge Tuohy needle.
Angle PJ, Kronberg JE, Thompson DE, Ackerley C, Szalai JP, Duffin J, Faure P. Dural tissue trauma and cerebrospinal fluid leak after epidural needle puncture: effect of needle design, angle, and bevel orientation. Anesthesiology 2003 Dec; 99(6): 1376 -82.
Electron microscopic analysis of particles from surgical gloves and their possible introduction into the epidural space during epidural anesthesia
Particles adhering to gloves can be drawn into the epidural space during continuous epidural anesthesia. All unnecessary manipulation should therefore be avoided, and the portion of the catheter to be inserted into the epidural space should not be touched in order to prevent possible nonspecific meningeal inflammatory responses.
Reina MA, Lopez Garcia A, Aguilar JL, Palacios Martin R. Electron microscopic analysis of particles from surgical gloves and their possible introduction into the epidural space during epidural anesthesia. Rev Esp Anestesiol Reanim. 1999 Feb; 46(2): 60 -6
From the skin to the epidural space
The distribution of distance from the skin to the epidural space in obstetric patients (n=2, 123) was: < 3 cm - 0. 3%; 3 to < 4 cm - 15%; 4 to < 5 cm - 47. 3%; 5 to < 6 cm - 28. 6%; 6 to < 7 cm - 6. 9%; 7 to < 8 cm - 1. 4%; and > 8 cm - 0. 5%
The mean value of the distance from skin to the epidural space in term parturients is influenced by the patient`s position during epidural needle placement. It is 4. 44 ± 0. 82 cm in the sitting position and 5. 03 ± 1. 05 cm in the lateral position.
Spinal dura mater thickness at the lumbar region is 0. 5 mm.
Using magnetic resonance imaging (MRI) of 39 patients Westbrook et al. found that the depth of the extradural space at the level of T 12 is 0. 83± 0. 195 cm. Westbrook JL, Renowden SA, Carrie LES. Study of the anatomy of the extradural region using magnetic resonance imaging. Br J Anaesth 1993; 71: 495 -498
Cerebrospinal fluid is formed at the rate of 400 ml/day.
The average adult has a total of 120 to 150 ml of fluid, of which only 20 to 35 ml are in the spinal portion of the subarachnoid space. In parturients, this volume in the spinal canal is decreased.
Valsalva, in 1682, was the first to remark on the CSF when he cut open the spine of a dog and noticed the liquid "which in all its aspects resembles that which is found in the joints".
Meme et al. using an epiduroscope could visualize the pulsation of the dura synchronized to heart rate. Meme E, Amici M, Ricci L, Merletti F. Epidural space: anatomical living view. International Monitor on Regional Anaesthesia 1993; 96
The human dura mater shows its fibers neither longitudinally nor parallel directed. It has thin collagen fibers and thick elastic ones with wavy characteristics, grouped in ribbons or sheets.
Human dura mater, Epidural surface (x 3, 500)
CSEGA Each one of the three kinds of anesthesia (spinal, epidural, general) has its advantages and disadvantages. A new concept of combined spinal-epiduralgeneral anesthesia (CSEGA) is illustrated with the objective of producing a new kind of anesthesia.
CSEGA is a new concept in anesthesia. The mixing of regional anesthesia with general anesthesia affords the anesthesiologist the opportunity to lower the local anesthetic doses and avoid using many kinds of intravenous drugs.
Zoric S, Stamenkovic D, Stevanovic S, Malenkovic V, Dikic SD, Randelovic T, Bilanovic D. Combined spinal epidural and general anesthesia in abdominal surgery. Med Arh. 2003; 57(4 Suppl 1): 21 -8
"All evolution in thought and conduct must at first appear as heresy and misconduct“ George Bernard Shaw (1856 -1950)
For Example: …
THANK YOU