Diabetes and Feet Zabeer Rashid Specialist Podiatrist Diabetes

Diabetes and Feet Zabeer Rashid Specialist Podiatrist - Diabetes

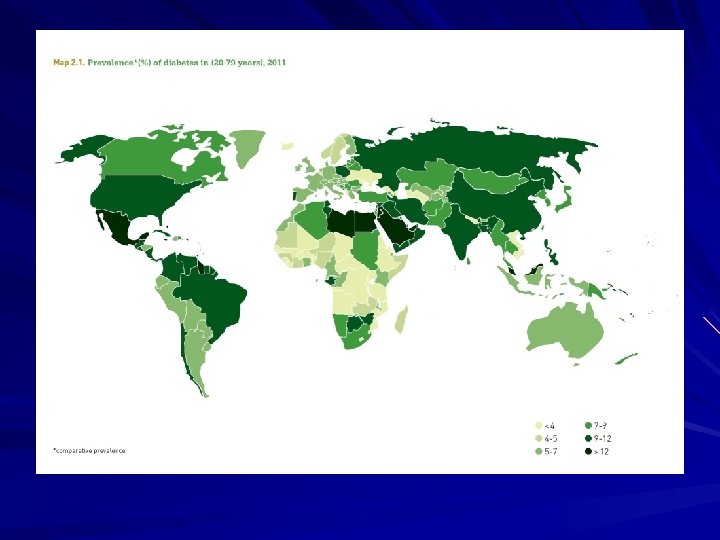
The rising tide of diabetes In the UK there are now 4. 50 million living with diabetes (3. 5 million with the diagnosis and 1 million with undiagnosed Type 2) Diabetes is now the single biggest cause of amputation, stroke, blindness and end stage kidney failure. Current spending accounts for around 10% of the NHS budget. ( Diabetes UK )

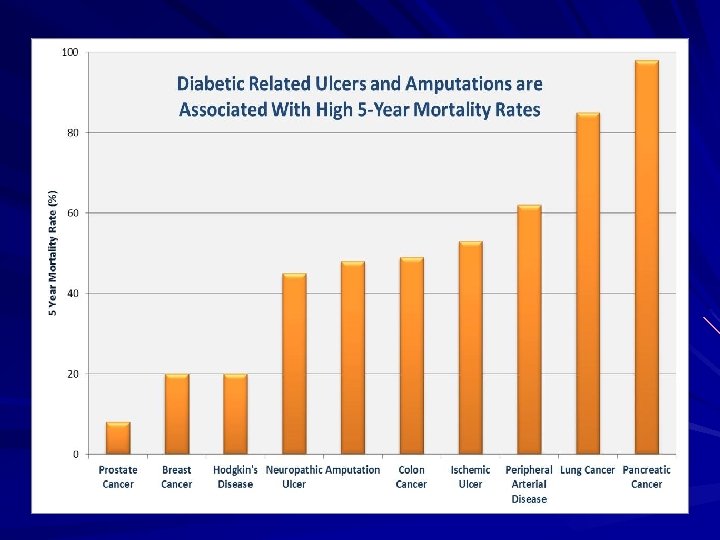
Diabetes and feet in numbers Foot complications are one of the most common reasons why a patient with diabetes will be admitted to hospital. ( Edmonds et al 1999 ) Around 7, 400 people with diabetes undergo leg, foot or toe amputation every year in England, about 140/week. (Public Health England) Only 50% of people with diabetes who have an amputation survive for 2 years. (Putting Feet First) The relative likelihood of death within 5 years following amputation is greater than for colon, prostate and breast cancer. (Putting Feet First)

Diabetes and feet in numbers It is estimated that 61, 000 people with diabetes in England have foot ulcers at any given time. Between 70% – 90% of all lower limb amputations are preceded by an ulcer.

Complications of diabetes Macrovascular Microvascular Ischaemic Heart Disease IHD Cerebrovascular Disease CVD Periperal Vascular Disease PVD Retinopathy Nephropathy Neuropathy

Vascular Assessment This is carried out to ensure there is an adequate blood supply to the feet. It involves feeling two pulses in each foot. Poorly controlled diabetes can reduce blood supply to the feet (ischaemia) causing delayed healing of wounds.

Vascular Assessment

Vascular Assessment

Vascular Assessment A hand held Doppler can be used to confirm the presence of pulses. Used with a sphygmomanometer the brachial and ankle systolic pressures can be measured. The ratio of ankle to brachial gives the pressure index ( ABI ). ABI score disease >1. 0 0. 75 -0. 9 0. 4 -0. 75 <0. 4 Suggested level of peripheral arterial None ( ? Calcified arteries ) Mild Moderate Severe

Neurological assessment SENSORY MOTOR AUTONOMIC
 Loss of vibration Loss of proprioception")
Sensory neuropathy Loss of pain (small fibre neuropathy) Loss of vibration Loss of proprioception Loss of touch Loss of temperature (small fibre neuropathy) Reduced/absent tendon reflexes RESULT: Lack of protective pain sensation ( A small number of patients have a small fibre neuropathy with impaired pain and temperature perception but with intact touch and vibration ).

Motor neuropathy Denervation of leg and foot muscles atrophy and paralysis/weakness = flexion deformities Reduction/loss of tendon reflexes Extensor plantar response ( +ve Babinski’s sign ) Cavus deformity of arch Prominent metatarsal heads New areas of increased pressure = greater risk of ulcer formation.

MOTOR Clinical signs High arch, prominent met. heads, proximal muscle wasting/atrophy. Also weakness when walking or climbing stairs. Clinical Tests Assessment of muscle power Assessment of muscle tone Limb reflexes - Patellar - Ankle Testing reflexes tests the sensory and the motor system at that level.


Autonomic neuropathy Autonomic function involves innervation and co-ordination of organs and the maintenance of homeostasis. Clinically; Dry skin with fissuring Loss of sweating Bounding pulses Distended veins (A-V shunting) Postural hypotension/faints

The Annual Foot Check All patients with diabetes should have an annual foot check as part of their care planning. These foot checks will primarily be carried out at the GP surgery by the GP/Practice Nurse/Health Care Assistant (HCA). It is vital that those who examine feet to determine risk status have the necessary training and competence. An essential part is patient education. The person with diabetes should be aware of the results of the examination and where to go in a potential emergency. There is a rolling programme of training in Tower Hamlets to ensure the person carrying out this vital check is competent.

What happens at a foot check Vascular assessment Neurological assessment Foot inspection Footwear Risk status Education Emergency advice

Neurological assessment SENSORY Burning sensation Hot and cold sensation Numbness Pins and needles Tightness Heightened awareness of sensation Lancinating pains

Neurological assessment SENSORY Light touch Cotton wool; 10 g Monofilament Vibration 128 Hz tuning fork; Neurothesiometer (when applied to foot delivers vibratory stimulus, which increases as voltage is raised. If unable to feel 25 v stimulus then at risk of ulceration) Proprioception Movement Temperature Warm/cold tubes Pain Neuropen/Neurotip

Vibration perception

10 g Monofilament

. PLANTAR ASPECT OF FEET Demonstrate on hand. Ask patient to close their eyes and respond ‘yes’ each time they feel it. Apply perpendicular to skin for 1. 5 -2 s. Do not apply to callus, scar tissue. Patient is ‘at risk’ if they score 8 or less out of a total of 10 test sites . .

Foot inspection The foot should be fully inspected including the top, sole, back of the heel and in between the toes. Colour; normal red & hot – may indicate infection, cellulitis dusky red, mottled or blue/cyanotic indicating ischaemia Skin; callus or corns dry, cracked – especially around heels moist, split in between toes open wounds, blisters, ulcers
, if patient or")
Foot inspection Nails; thickened and or involuted ( excessive curvature ), if patient or carer managing then NO need to refer to Foot Health but encourage continued self-care

Footwear Foot shape; observe for deformity such as bunions, clawed toes, very wide or swollen feet that would make shoe fitting difficult with standard footwear. Shoes; ideally should be soft leather uppers with fastening – laces/velcro check for suitability, does foot show signs of shoe pressure (eg corns or callus) are there signs of bulging ( narrow toe-box ) is the style suitable for daily wear?

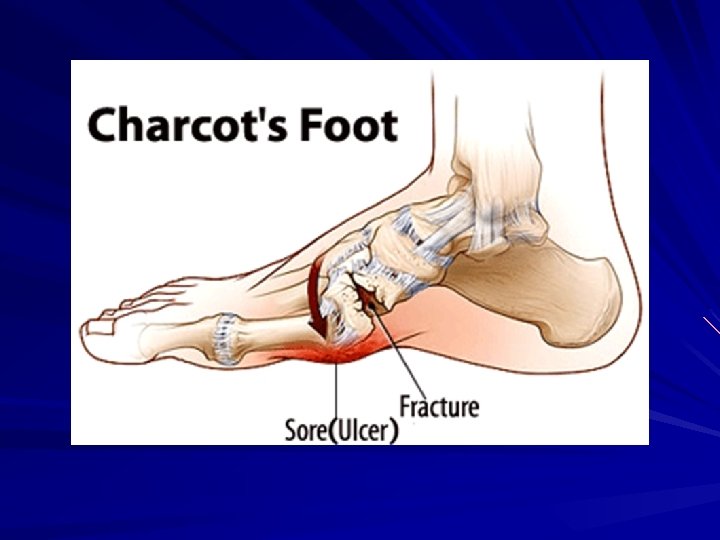
Charcot Foot The term Charcot refers to bone and joint destruction that occurs in the neuropathic foot. Acutely there is unilateral erythema, oedema and the foot is much warmer, essentially a red, hot and swollen foot. Typically there are no open lesions on the affected foot. There may be a history of trauma, sprain or strain injury. Early diagnosis is essential to reduce risk of bony destruction and deformity>’rocker bottom’ foot. Refer immediately to the Emergency Foot clinic.

Education Check Feet Daily Use emollient on dry skin Cut nails carefully/file all edges Never use corn plasters/blades Wear correctly fitting shoes Clean hosiery daily Seek help immediately if problems Make aware of emergency foot clinic Reassure
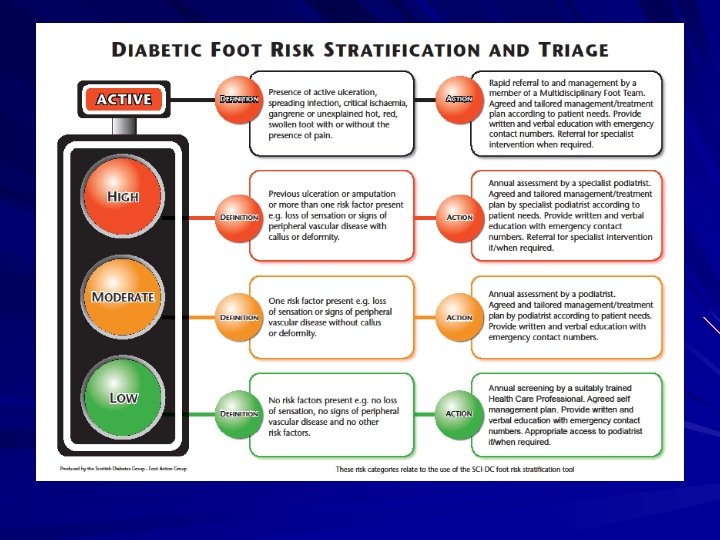

1 -4% ULCERATED 4 -8% PATIENTS AT HIGH RISK 20% PATIENTS AT MODERATE RISK 70% PATIENTS AT LOW RISK

Care in an Emergency All patients with diabetes MUST be aware of what to do in an emergency and where to go. In an ideal world the patient will always self-refer in a potential emergency! Emergency conditions Discharge; blood/pus/clear fluid. Sudden redness/heat/swelling whether painful or not. Infection New wound/injury

Emergency Foot Clinic If you notice any of the emergency conditions or are unsure please attend our Emergency Foot Clinic. This is open from Monday→Friday. You must be there for 8. 30 am. You do not need an appointment or referral. Go to the Department of Foot Health. 2 nd Floor, Mile End hospital. At weekends go to A+E. ANY DELAY IN SEEKING ADVICE/TREATMENT CAN LEAD TO WORSE OUTCOMES. TIME IS TISSUE!

Department of Foot Health Mile End hospital Bancroft Road London E 1 4 DG FOOT HEALTH SERVICE EMERGENCY CLINIC Monday to Friday – 8. 30 am prompt (Excluding Bank Holidays) No appointment necessary for the emergency conditions shown below Blisters, sores Discharging wounds Swollen/inflamed areas Sudden injuries

SITE REFERRAL METHOD CONTACT DEPARTMENT OF FOOT HEALTH MILE END HOSPITAL BANCROFT ROAD LONDON E 1 4 DG TEL: 0208223 8849 FAX: 0208 223 8941 LETTER OR FAX FOR NONURGENT REFERRALS OFFICE MANAGER DIABETES CARE CENTRE MILE END HOSPITAL BANCROFT ROAD LONDON E 1 4 DG TEL: 020 8223 8836 FAX: 020 8223 8806 CLINIC IS FOR CARE OF DIABETICS WITH ACTIVE FOOT DISEASE, CANNOT REFER IN TO DIRECTLY – USE EMERGENCY CLINIC SITES; DEPARTMENT OF FOOT HEALTH MONDAY - FRIDAY PATIENT MUST ARRIVE AT 8: 30 AM EMERGENCY CLINIC IS FOR; • OPEN WOUNDS/BLISTERS • INFECTION • DISCHARGE BLOOD/PUS • SUDDEN INJURIES • SWOLLEN OR INFLAMED AREAS PODIATRISTS; VICTORIA GRIFFIN ZABEER RASHID ANITA MCCALLA STEPHANIE BENJAMIN CLINICIAN ON DUTY

DON’T BE DE-FEETED BY DIABETES!

zabeer. rashid@elft. nhs. uk
- Slides: 38