Concepts of Continuous Renal Replacement Therapy in Adult



















 ▫ 50 x 24=1200")




")

 calcium")


- Slides: 30
Concepts of Continuous Renal Replacement Therapy in Adult critical care at LTHT Including: Anticoagulation Prescribing Protocol
Introduction • The machine used at Leeds Teaching Hospitals to deliver Continuous Renal Replacement Therapy (CRRT) is the Fresenius Multi. Filtrate machine • The mode of treatment we use is continuous veno-venous haemodialysis (CVVHD) • The first line anticoagulation is Regional Citrate Anticoagulation (RCA)
Indications for CRRT INDICATIONS • • • High serum potassium Acidosis Pulmonary Oedema Control of uremic symptoms Hyperpyrexia Filter metabolites/Septic mediators • Drug poison removal WHEN TO USE • Hyperkalaemia k⁺ >6. 5 mmol/L • Metabolic Acidosis Ph <7. 1 • Pulmonary Oedema (not responsive to diuretics) • Uremic Encephalopathy/Neuropathy • Non emergency initiation ▫ Fluid management ▫ Solute control ▫ Pre-existing ESRF • Lactate is not removed by dialysis
CVVHD • During CVVHD diffusion of molecules takes place between blood in one fluid compartment of the dialyser and dialysis fluid in the other fluid compartment • Haemodialysis utilizes counter current flow where the dialysate is flowing in the opposite direction to blood flow in the extracorporeal circuit • Counter-current flow maintains the concentration gradient across the membrane at a maximum and increases the efficiency of the dialysis
Anticoagulation • Anticoagulation of blood is required to avoid clotting in the filter circuit • The default choice of anticoagulation at Leeds is Regional Citrate Anticoagulation (RCA) • This reflects a change from historic practice where heparin was used • RCA offers longer filter life and may reduce complications, it also avoids systemic anticoagulation
Alternative anticoagulation options • Unfractionated heparin • None if INR >2. 5 and platelets <80 • Prostacycline used rarely
Regional Citrate Anticoagulation • • Negatively charged ion Binds with ionised calcium Forms a single negatively charged chelate complex Concentration of free ionised calcium in blood is reduced in the circuit • Ionised calcium is essential to the coagulation cascade – reducing it reduces clotting • Some of the citrate-calcium complex is removed by the filter and rest passes into patient where it is metabolised by the liver
Regional Citrate Anticoagulation • Clotting cascade cannot function if ionised calcium in bloods falls <0. 5 mml/L • <0. 3 mmol/L clotting abolished • Target calcium concentration in the circuit for optimal function is 0. 25 -0. 34
Fresenius Multifiltrate • This is the machine used in Leeds • It can be used with RCA or heparin • Ci-Ca is the system for RCA • Multibic with heparin (separate protocol)
Fresenius Ci-Ca system 4 3 5 2 1
Fresenius Ci-Ca System • 4+2 pump-system • Citrate infusion is coupled to the blood flow • Citrate and calcium infusion is automatically taken into account for fluid balancing • Dedicated Zero-Ca, Low. Bicarb dialysate and Ci-Ca cassette with pre-connected citrate and calcium lines
Fresenius Ci-Ca System
Dialysate Fluid • Sodium and Bicarbonate reduced in order to compensate for the systemic infusion of Sodium Citrate • Calcium free to avoid unnecessary increase of citrate requirements. • It is a double chamber bag • Fluid is stable for 24 hours once mixed • At Leeds we only use K⁺ 4 mmol/L bags if patient has hyperkalaemia use 35 m. L/Kg/Hr dialysis dose Fluid Constitution Na⁺ K⁺ Mg⁺⁺ Ca⁺⁺ HCO 3⁺ Cl⁻ Glucose 133 mmol/L 4 mmol/L 0. 75 mmol/L 0 mmol/L 20 mmol/L 116. 5 mmol/L 1 g/L
Core safety concepts • Protocol must be followed • Prescription must be written before patient connected to system and then daily • RCA interferes with normal calcium homeostasis maintain a safe serum ionised calcium level
Core safety concepts • Safety check via T: I ratio – this is the total: ionised calcium ratio and is a marker of citrate accumulation • RCA interferes with acid-base balance - be aware that the blood flow and dialysate flow need to be balanced (1: 20 ratio) to prevent iatrogenic acidosis or alkalosis • Liver patients may not tolerate RCA – separate guidance
Limits • Maximum treatment duration is 120 hours per filter • Washback, recirculation and disconnection circuit can be reconnected up to four hours • Recirculation with blood – circuit can be reconnected up to 30 mins
Dose choice • Dialysis dose can be chosen as 25 ml/kg/hr or 35 ml/kg/hr – weight based guidance charts in protocol • 25 is the default choice • 35 should be chosen in patients with: ▫ ▫ Severe hyperkalaemia (>7 mmol/l) Severe acidosis (p. H <7. 0) Ethylene glycol poisoning Inadequate treatment on 25 ml/kg/hr
Calcium Management • Refer to the protocol for guidance in calcium management • Around 60% of patients in critical care need to be pre-treated with calcium • Be mindful that in all patients the systemic ionised calcium will drop in the first 24 -48 hours, this is not a citrate accumulation unless the T: I ratio is > 2. 5 • Calcium management is the single most important factor of citrate anticoagulation
Fluid management • CRRT is a powerful tool for correcting fluid balance • Prescription should state a range of removal rates and a target fluid balance • Start the removal rate based upon current input and target balance and adjust in response to changes over the course of the day
Fluid management example • Hourly input total 50 ml (propofol/alfentanil/feed) ▫ 50 x 24=1200 • Anuric, no drains/loose stools etc • Target balance –ve 1000 ml/24 hours • Set initial removal at 100 ml/hr (approximated) ▫ 1200+1000=2200 ▫ 2200/24=92 • After 12 hours patient given 500 ml blood ▫ Balance, before blood, at 12 hours is -600 ml [(50 x 12)-(100 x 12)] ▫ After blood is -100 ml with 12 hours left, input still 50 ml/hr ▫ Aim remains -1000 ml • Set removal at 125 ml/hr ▫ -100 + (50 x 12) = +500 ▫ 500+1000=1500; 1500/12=125
Acid-Base Management • Citrate is metabolised in the liver • The by-product of citrate metabolism is bicarbonate • One molecule of citrate produces 3 molecules of bicarbonate • You require a prescription at a 20: 1 (dialysate flow: blood flow) ratio to maintain homeostasis • Any derangement in acid-base must be assessed to ascertain if it is a due to patient pathology or due to the RCA itself
Metabolic acidosis potential causes • Is it the patients underlying condition? • Has therapy been running long enough? • Inadequate dialysis dose? May need to increase dialysis to 35 m. L/kg/hr • Dialysate flow rate too high in relation to blood flow rate, i. e. not 20: 1 (was the prescription previously written for metabolic alkalosis? ) • Citrate accumulation due to impaired metabolism. T: I ratio will be >2. 5
Prescribing for Metabolic Acidosis Either: • Decrease dialysate flow ▫ Less removal of citrate by filter therefore effectively increased bicarbonate delivered to patient • Increase blood flow (increases citrate flow) ▫ More citrate delivered to system without increased removal by filter, therefore also effectively increasing bicarbonate delivery • Could consider increasing dialysis to 35 m. L/kg/hr ▫ Increased dose of dialysis will aid clearance of pathological acidosis This should be done if there is no other reason for the patient to be acidotic.
Metabolic alkalosis potential causes • Check patients underlying condition • Dialysate flow rate too low in relation to blood flow rate (<20: 1) • Check for medications that may cause alkalosis • Filter age ▫ As treatment continues the filter slowly blocks resulting in reduced clearance and a greater proportion of citrate reaching patient ▫ This increased delivery of citrate is converted to bicarbonate
Prescribing for Metabolic Alkalosis • Decrease blood flow (this should be the first action) ▫ Decreased citrate into the system so effectively less bicarbonate delivered to patient • Increase dialysate flow ▫ Increased clearance of citrate by filter so effectively less bicarbonate delivered to patient • Consider changing the filter set if >72 hours old This should be done if there is no other reason for the patient to have an alkalosis
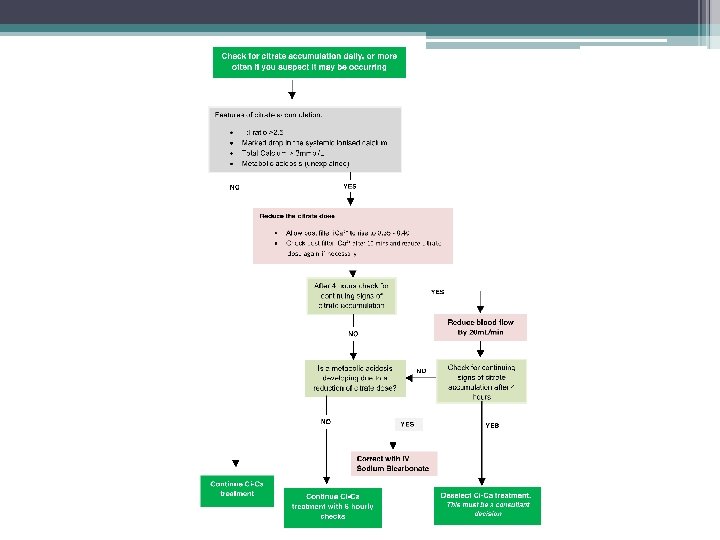
Citrate Accumulation • Problems may occur if the patient is unable to adequately metabolise citrate in the presence of acute severe liver failure and/or severe lactic acidosis • Signs include ▫ ▫ T: I ratio >2. 5 Marked drop in systemic Ca 2+ Elevated total calcium (>3) Anion gap acidosis • Protocol dictates management if suspected
Liver Patients • Altered protocol if lactate >8 and total to ionised (TI) calcium ratio >2 ▫ Always pretreat with calcium ▫ Increased initial calcium flow rates • At increased risk of citrate accumulation. Vigilance required
Summary • Main indications for CRRT are hyperkalaemia, acidosis or fluid overload • Anticoagulation is usually with citrate which works by binding to ionised calcium which prevents activation of the clotting cascade • You must monitor and control patients and filters Ca 2+ levels • Fluid balance targets must be adhered to • Be aware that the system can both cause and correct an acid-base imbalance • T: I ratio is an essential safety check – risk of citrate accumulation
Points of contact • Charlotte Trumper – Clinical Nurse Specialist • James Beck – ICM Consultant • Andy Lewington – Renal Consultant