C S F RHINORRHEA Lt Col Mian Amer






 Hydrocephalus Normal pressure")

























- Slides: 34
C. S. F RHINORRHEA Lt Col Mian Amer Majeed Classified ENT Specialist MH Rawalpindi
INTRODUCTION It is the failed containment of the cerebrospinal fluid in the subarachnoid compartment. n It indicates a communication with the subarachnoid space & therefore an opening of the arachnoid, the dura and the bone to permit exit of the CSF through the nose. n
Cont…. n The actual loss of CSF is of no particular consequence however the persistent dural fistula represents a persistent hazard for a potentially fatal purulent meningitis leading to death if unrecognized. n Persistent CSF rhinorrhea is therefore an absolute indication for a surgical repair of the leak.
ORIGIN Origin may be from any cranial fossa i. e Anterior, n Middle, or n Posterior n
CSF PRESSURE n Normal CSF pressure is 40 mm in infants & 140 mm in adults.
CAUSES OF CSF RHINORRHEA n TRAUMATIC Accidental Acute Delayed Iatrogenic Acute Delayed
Cont…. n NON TRAUMATIC High pressure Tumours (direct/ indirect effect ) Hydrocephalus Normal pressure Congenital anomalies Focal atrophy of olfactory/sellar area Osteomyelitic erosion Idiopathic
CAUSES…. Traumatic 80 %. . secondary to head trauma with associated skull base #. n 16%. . operations on nose , paranasal sinuses, skull base. n Mostly occur through anterior cranial fossa. As the bone of the anterior skull is thin & densly adherent to the dura so dural tears also occur. n
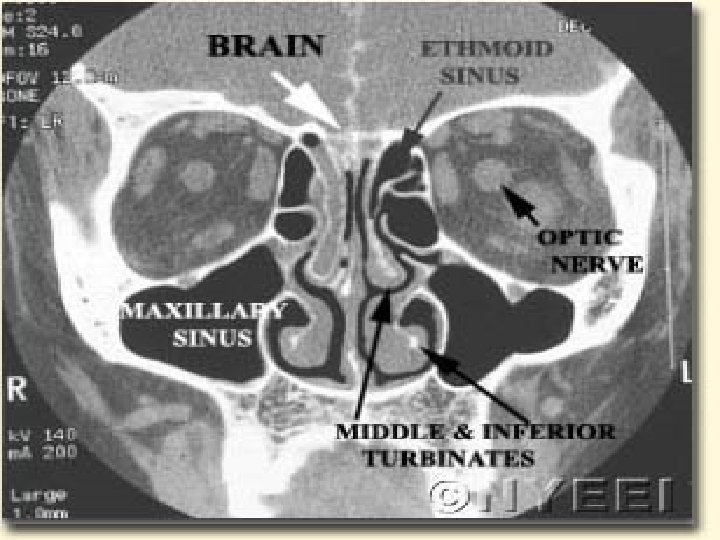
Cont…. n Sites commonly involved in the anterior cranial fossa are Cribriform plate (commonest ) Fovea ethmoidalis Posterior wall of frontal sinus
Cont…. n Middle cranial fossa fractures are less likely to cause CSF leakage into the nose however common routes are Via the sphenoid sinus Eustachian tube
Cont…. n CSF rhinorrhea may occur from the posterior fossa in fractures of Clivus Petrous temporal bone
Cont…. Post traumatic CSF rhinorrhea is immediate in most of the cases n When delayed, it appears within 3 months in 95% cases, probably due to initial inflammation & edema resorption of bone/soft tissue disrupted blood supply weakening of pia arachnoid seal n
NONTRAUMATIC CAUSES Uncommon n Mostly in adults n 4 th decade n ♂ : ♀ ratio is 1: 2 n May occur after an episode of coughing, sneezing or straining. n
High pressure leaks Arise from the cribriform area in 75 % of cases n They act as a safety valve to decrease the raised ICP n 84% are associated with slow growing intra cranial tumours (Pituitary neoplasms are the commonest) n 16 % are related to hydrocephalus n
Normal pressure leaks Mostly are from the cribriform area and the sella turcica but may be from the middle fossa. n 90 % are due to potential congenital pathways n 10 % are due to direct erosion of skull base due to infections/ tumours like Osteomas of the fronto ethmoidal region, Nasopharyngeal angiofibromas, Nasopharyngeal CA, Osteomylitic erosion n
Diagnostic Aims n Is the fluid CSF? n Cause of leakage n Site of leakage
Presence of CSF leak n History In cases of trauma any persistant rhinorrhea should be considered CSF until proved otherwise. Patient with recurrent pneumococcal meningitis Bending the head forward will increase the rate of flow Headache Salty taste Anosmia Associated Symptoms
Cont… Examination May be unremarkable except for the rhinorrhea. Positional change or jugular compression can increase the flow Reservoir sign: After being supine for sometime the patient is brought in an upright position, with the neck flexed. A sudden rush of clear fluid is indicative of CSF fistulae. n
Cont…. Hankerchief Test: Fluid in rhinitis contains mucous which stifins while CSF doesnot. n Halo Sign: When CSF rhinorrhea is blood stained it dries out with a central blood stain surrounded by a clear ring. n Nasal endoscopy with or without intrathecal floresein for leak presence or localization n
Cont…. . Biochemistry/ Immunochemistry Estimation of glucose, proteins and electrolytes can be done. A concentration of 30 mg/dl or 1. 6 mmol/l of glucose is considered confirmatory of CSF, however active meningitis can lower the CSF glucose level. n β-2 Transferrin is pathognomonic of CSF n
Demonstrate the Cause Over ½ the cases of nontraumatic rhinorrhea are high pressure leaks, majority related to intracranial tumours. n CT scans and MRI have their diagnostic role n
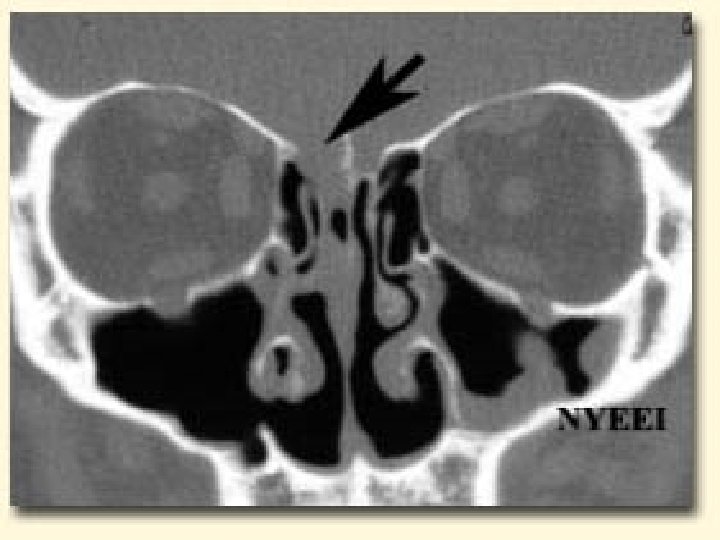
Localization of the leak Radiology plays the key role to see the anatomical site, size, side of the fistula n Bone defects, air fluid levels and erosions can be seen. n Plain X rays… Pneumocephalus/ air fluid levels n CT scan in axial/ coronal views… Skull Base #s, CSF fistulae n MRI… is not used as it is unable to show bone windows n
Cont… n Isotope studies In case of inactive, intermittent, small or doubtful leak, CT scan with contrast will not reveal the leak. In such cases radio nuclied cisternography is more effective. Indium III- DPTA is generally used.
Cont… n Intrathecal dyes Intrathecal floreciene with nasal endoscopes are used for anterior fossa leaks
Management n Management consists of cooperation between Neurosurgeon Neuroradiologist Otolaryngologist depending upon severity, etiology, extent of injury & anatomical site of leak.
Cont…. Treatment can be divided into Medical & Surgical MEDICAL In the acute CSF leak an initial trial of conservative treatment should be considered as majority of acute traumatic leaks heal spontaneously. n
Cont…. Bed rest in head up position n Avoiding coughing, sneezing, nose blowing & straining. n Drugs to decrease spinal fluid production like acetazolamide and frusemide. n Repeated removal of CSF via lumbar taps or an indwelling lumbar subarachnoid drain. n Antibiotics n
Cont…. n If conservative treatment fails after 10 to 14 days or if the leak recurs then surgical treatment is indicated.
Surgical management Intracranial approach n Extra cranial approach n Endoscopic repair n
CSF rhinorrhea? Confirm presence of leak History examination Traumatic/Atraumatic Nasal endoscopy conservative failure localization Surgical closure successful Glucose/ β 2 transferrin
Thank you