AUTOIMMUNE IMMUNE DEFICIENCY DISORDERS AUTOIMMUNITY Immune reactions against












 • Primary Biliary")
 in")


 and")
 • • Characterized by Chronic Inflammation thought to be result of autoimmunity")







- Slides: 33
AUTOIMMUNE & IMMUNE DEFICIENCY DISORDERS
• AUTOIMMUNITY: Immune reactions against self antigens
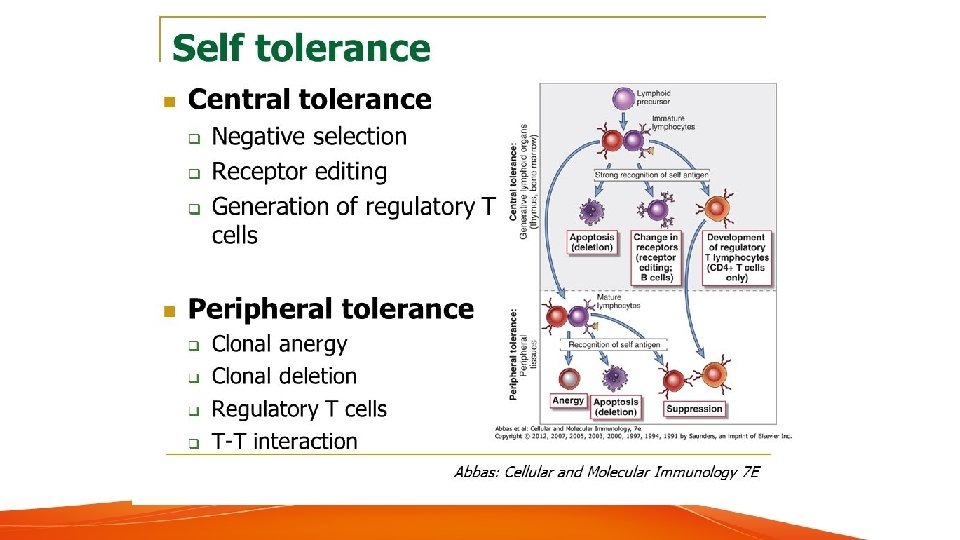
IMMUNOLOGIC TOLERANCE • Phenomenon of being unresponsive to an antigen induced by exposure of lymphocytes to that angtigen. • Normal/All Good • Self Tolerance: lack of responsiveness to an individuals own antigens. • Normal/All Good
IMMUNOLOGIC TOLERANCE DIVIDED IN 2 • CENTRAL TOLERANCE • PERIPHERAL TOLERANCE
CENTRAL TOLERACNE • Immature self reactive T and B Lymphocytes clones that recognize self antigens during their maturation in the central lymphoid organs( thymus for the T cells and bone marrow for the B Cell) are killed or rendered harmless.
CENTRAL TOLERANCE----T cells • Negative Selective or Deletion: When T Cells that recognize self antigens(TCR) in the Thymus they die by apoptosis. • Protein Called Autoimmune Regulator (AIRE) Stimulates expression of some peripheral tissue restircted self antigens in the thymus which is critical to kill those immature T Cells sensitive for those tissue antigens.
CENTRAL TOLERANCE---B CELLS • RECEPTOR EDITING: In Bone Marrow, when B Cells are developing. If they react with self antigens the machinery for Antigen Receptor Gene Rearrangement occurs and new antigen receptors are formed. Almost half of B Lymphocytes go through this mechanism. • APOPTOSIS: If receptor editing does not occur, these reactive B lymphocytes die via apoptosis.
• CENTRAL TOLERANCE IS NOT PERFECT. • THERE IS SOME SLIPPAGE OF SELF REACTIVE B AND T LYMPHOCYTES • THEY WILL BE TAKEN CARE OF BY PERIPHERAL TOLERANCE.
PERIPHERAL TOLERANCE • ANERGY: Lymphocytes that recognize self antigens may rendered functionally unresponsive by expressing CTLA 4 which bind with B 7 molecules on APCs and reduce their ability to activate T cells via CD 28. • SUPPRESSION BY REGULATORY T CELLS: secrete IL -10 and TGF-B which inhibit lymphocyte activation nd effector functions. Also express CTLA 4. • DELETION VIA APOPTOSIS: Through Bim and Fas-Fas Ligand System.
MECHANISMS OF AUTOIMMUNITY • DEFECTIVE TOLERANCE OR REGULATION • ABNORMAL DISPLAY OF SELF ANTIGENS(stress and injury). • INFLAMMATION OR AN INITIAL INNATE IMMUNE RESPONSE(microbes or cell injury) • ROLE OF SUSCEPTIBILITY GENES(HLA B 27/MHC genes)(PTPN 22/Non MHC in RA)(NOD 2/Non MHC in Crohns) • ROLE OF INFECTION (molecular mimicry)(breakdown anergy).
DISEASES MEDIATED BY ANTIBODIES • ORGAN SPECIFIC • Autoimmune Hemolytic Anemia • Autoimmune Thrombocytopenia • Myasthenia Gravis • Graves Disease • Goodpasture Syndrome • Autoimmune Atrophic Gastritis of Pernicious Anemia SYSTEMIC • Systemic Lupus Erthematosus
DISEASES MEDIATED BY T CELLS • Type 1 Diabetes Mellitus • Multiple Sclerosis • Rheumatoid Arthritis • Systemic Sclerosis • Sjogren Syndrome
DISEASES POSTULATED TO BE AUTOIMMUNE • Inflammatory Bowel Diseases(Crohns, Ulcerative Colitis) • Primary Biliary Cirrhosis • Autoimmune (Chronic Active) Hepatitis • Polyarteritis Nodosa • Inflammatory Myopathies
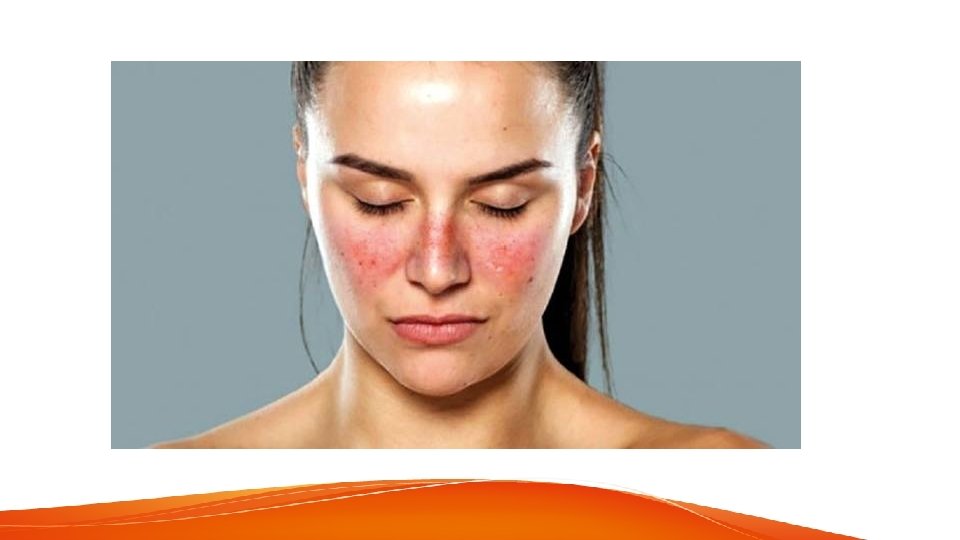
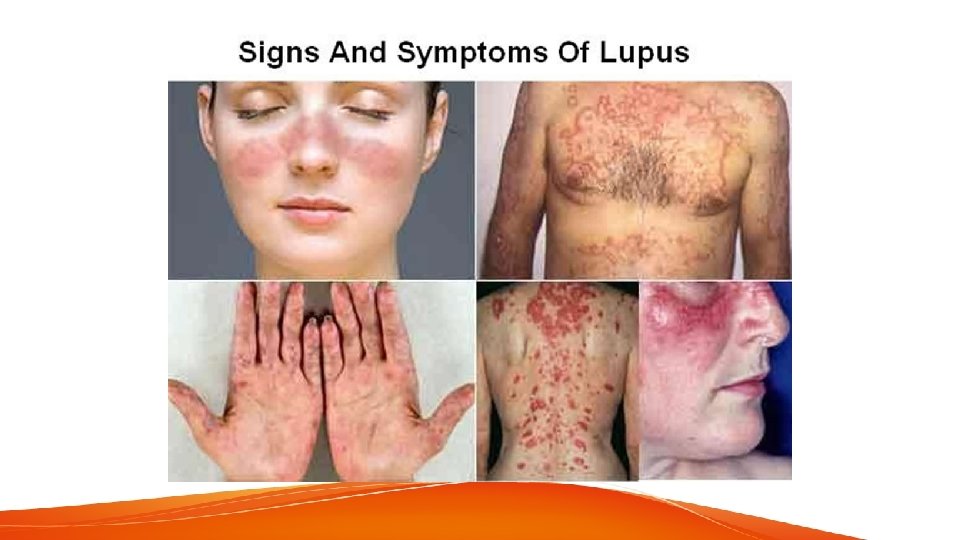
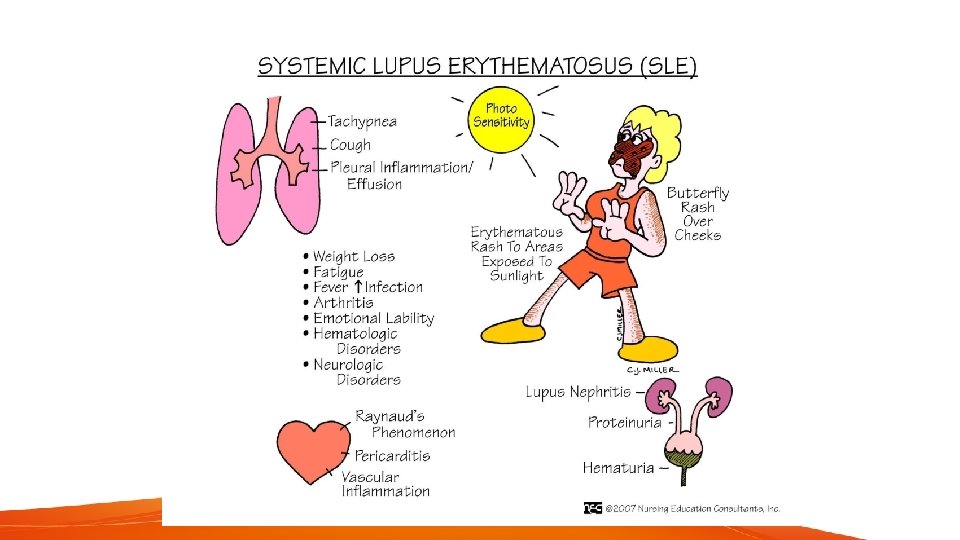
SYSTEMIC LUPUS ERYTHEMATOSUS • Autoimmune Disease involving multiple organs, characterized by autoantibodies (ANA) in which injury is caused by deposition of immune complexes and binding of antibodies to various cells and tissues. (Mixed Type 2 and 3 Hypersensitivity). • Cause: failureof mechanism that mantain self tolerance, Genetic factors of MHC and Non MHC Genes, Complement Deficiencies, Environmental Factors Like UV exposure and Drug induced by Hydralazine, procainamide.
SYSTEMIC LUPUS ERYTHEMATOSUS CLINICAL MANIFESTATION PREVELANCE IN PATIENTS % Hematologic 100 Arthritis, Arthralgia, Myalgia 80 -90 Skin 85 Fever 55 -85 Fatigue 80 -100 Weight Loss 60 Renal 50 -70 Neuro. Psych 25 -35 Pleuritis 45 Pericarditis 25 Gastrointestinal 20 Raynayd 15 -40 Ocular and Peripheral Neuropathy 5 -15
RHEMUTOID ARTHRITIS • Swollen, Painful, Warm Joints. Esp in Hands in Wrist. Weight Loss Stiffness. • Mediated by T Cells, Immune Complexes and Chronic Inflammation. • PIP and MCP frequently involved • Knee joint and MTP also. • Skin, Heart, Lungs and Eyes can also be involed.
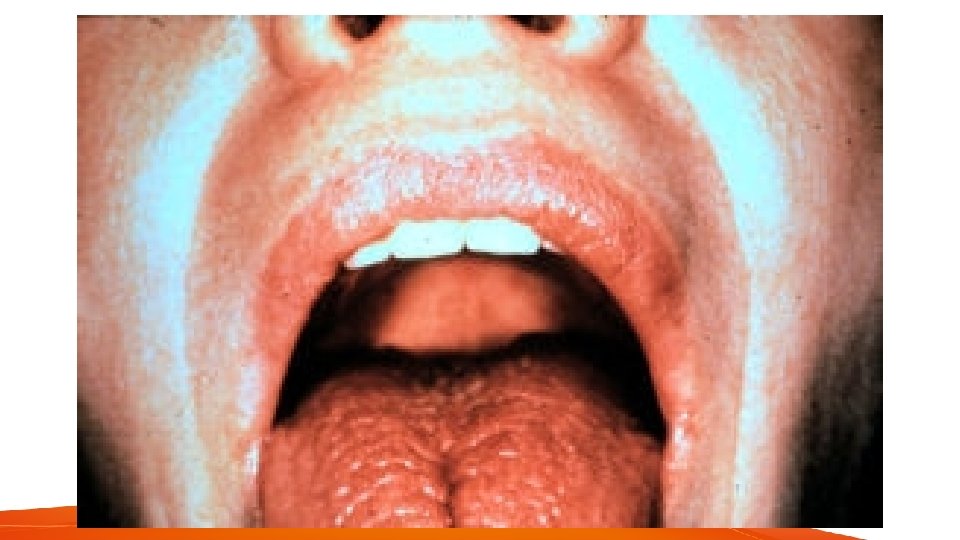
SJOGREN SYNDROME • Is a chronic disease characterized by dry eyes (keratoconjunctivitis sicca) and dry mouth(xerostomia) resulting from immunologic destruction of lacrimal and salivary glands • Mostly womman between 50 -60 years age • Biopsy of lip for diagnosis. • Antibodies SS-A , SS-B found which are against ribonucleoprotein antigens. • Associated with HLA Alleles and other auto immune disorders.
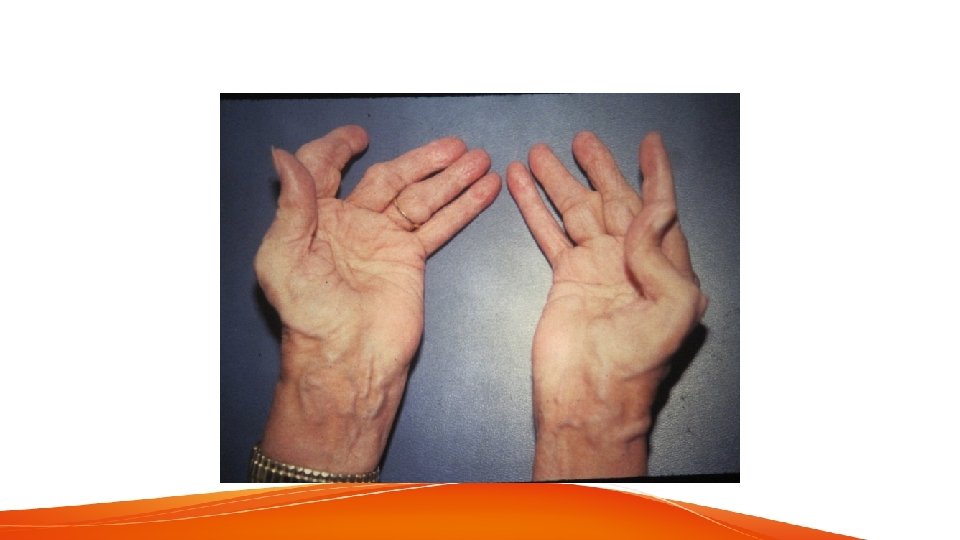
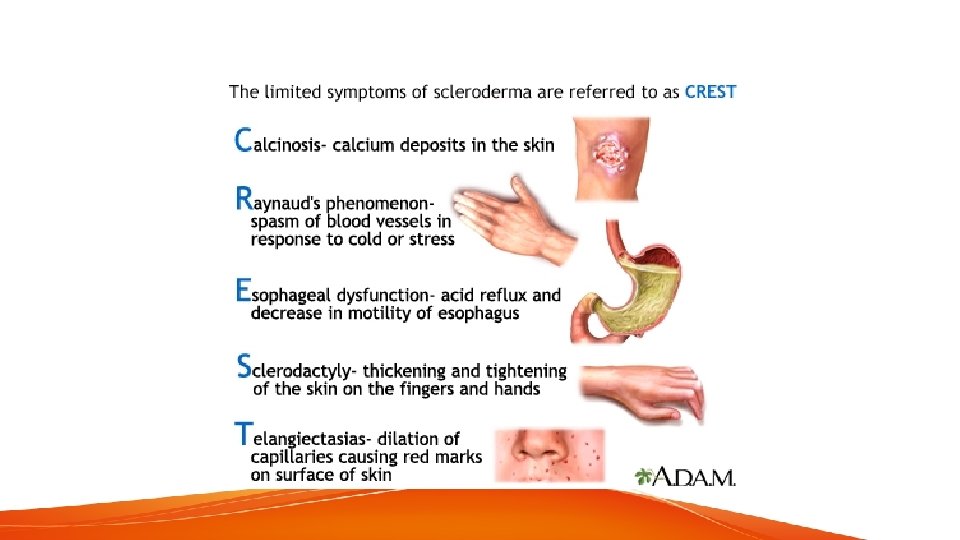
SYSTEMIC SCLEROSIS(SCLERODERMA) • • Characterized by Chronic Inflammation thought to be result of autoimmunity widespread damage to blood vessels progressive interstitiala nd perivascular fibrosis in skin and multiple organs. • Occurs in Skin, Alimentary Tact, Musculoskeletal System, Kidneys, Lungs nad the Heart.
TRANSPLANT REJECTIONS • Rejection: Process in which T Lymphocytes and antiboies produced against graft antigens react against adn destroy tissue grafts. • Major difference between a donor and recipient that result in rejection of tranplants are diffrences in HLA Alleles. • Allografts: Same species, Xenograft: different species • Rejection occurs via Direct or Indirect Pathway.
IMMUNODEFICIENCY SYNDROMES • Divided into Primary and Secondary • Primary: Genetic • Secondary: Acquired( comlications of cancer, infections, irradiation or chemotherapy of cancer and other diseases). • Increase in infections • Deficiencies in innate immunity include defects of phagocyte function, complenet and innate immune receptors.
Immunodeficiencies • X-SCID: Failure of T Cell and B Cell Maturation. Leading to defective lymphopoiesis • Autosomal recessive SCID: failure of T CEll Development • X-Linked agammaglubulinemia(XLA): Failure of B Cell Maturation, absense of antiboies, Mutation in BTK gene which encoes B Cell tyrosine Kinase, required for maturation signal from Pre B Cell and B cell Receptors. • Selective IGA deficiency • X-Linked hyper-ig. M syndrome. L failure to produce (ig. G, ig. A, ig. E 0 due to mutation in gene encoding.
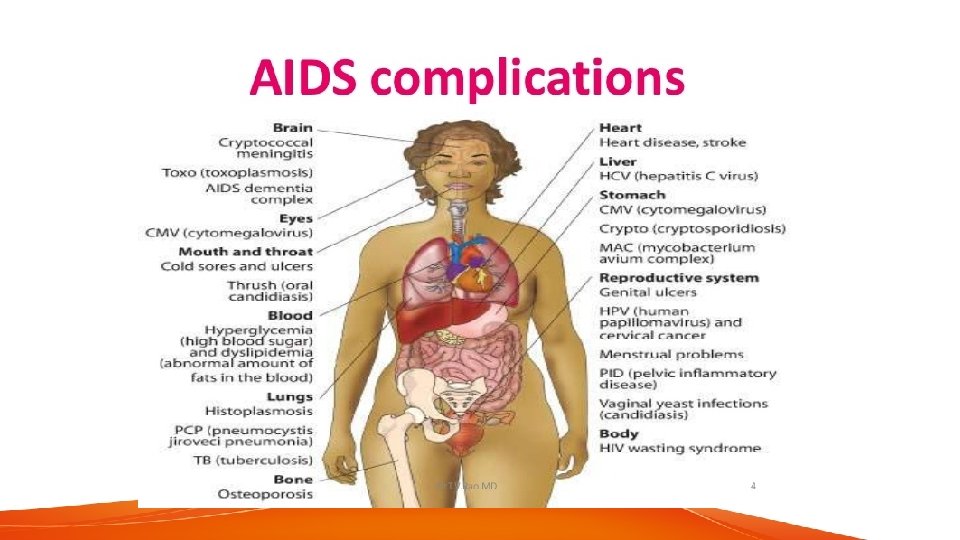
SECONDARY IMMUNEDEFICIENCIES • AIDS: Acquired Immunodeficiency Syndrome • Disease caused by retrovirus Human Immunodeficiency virus(HIV) and charactereized by profound immunosupression that leads to oppotunistic infections, secondary neoplasms and neurlogic manifestations. • Epidemiology: Homoesexual or Bisexual, IV Drug Abusers, Hemophiliacs, Heterosexual Contact, HIV Infection of newborn. • It is sexually transmitted, along with other fliuds, parenteral infection.
AIDS • Two main targets of virus: CNS and Immune System. • Profound immune deficiency particularly the cell mediated immunity. --> loss of CD 4 T Cells • Lymphoid tissues, Macrophages and dendritic cells also infected. virus spreads throughout the body and keeps changing its genetic makeup. • acrophages and microglia in Brain are also affected and HIV can induce damage in brain. • Final Phase of Infection is called AIDS
AIDS • Symptoms: • Fever, Weight loss, diarrhea, generalized lymphadenopathy, multiple opportunistic infections, neurologic disease and secondary neoplasms.
THANK YOU