APNEA OF PREMATURITY DR MIZERO S PATERNE CHIEF













 •")











- Slides: 28
APNEA OF PREMATURITY DR MIZERO S. PATERNE CHIEF REGISTRAR, PEDIATRICS Venue: Rwanda Military Hospital Date: April 19, 2018
OUTLINE 1. 2. 3. 4. 5. 6. 7. 8. 9. Background Definition and classification Causes of apnea Evaluation of a child with apnea Treatment of apnea Emergency treatment Methylxanthines Complications of AOP Surveillance AOP
1. BACKGROUND Apnea of prematurity : common in NICU Data suggest that a worse neurodevelopmental outcome > 36 weeks Inversely proportional to gestational age (GA)
2. DEFINITION AND CLASSIFICATION Apnea is usually defined as a cessation of breathing for a period equal or greater than 20 seconds or a shorter pause accompanied by bradycardia (<100 beats per minute), cyanosis, or pallor. However, in practice, many apneic events in preterm infants are shorter than 20 seconds, because briefer pauses in airflow may result in bradycardia or hypoxemia.
2. DEFINITION AND CLASSIFICATION • On the basis of respiratory effort and airflow, apnea may be classified as: 1. Central apnea (40%): no chest wall movement & airflow 2. Obstructive apnea (10%): presence of chest wall movement but no airflow. 3. Or mixed. Apnea (50%): central apnea is either preceded or followed by airway obstruction. The majority are mixed events, Often Ao. P reflects a ”physiological” immature state of respiratory control rather than a ”pathological” condition
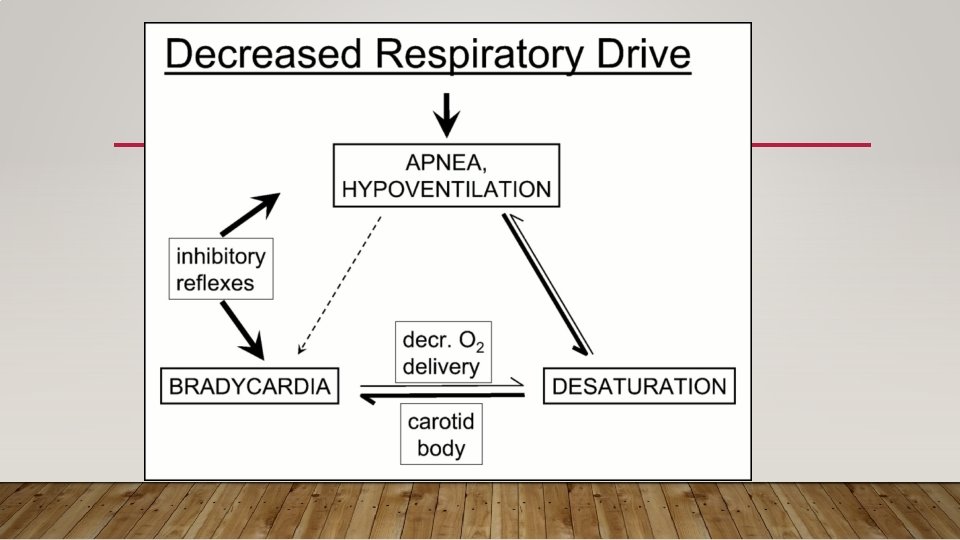
2. 1 CENTRAL APNEA •
2. 2 OBSTRUCTIVE APNEA • Pause in alveolar ventilation - obstruction of airflow within the upper airway (pharynx). • Once collapsed, mucosal adhesive forces tend to prevent the reopening of the airway during expiration. • Neck flexion will worsen this form of apnea. • Excessive secretions in the nasopharynx and hypopharynx may also cause obstructive apnea.
2. 3 MIXED APNEA • A combination of both types ~ 50% • Mixed apnea consists of obstructed respiratory efforts usually following central pauses. • Central apnea is either preceded or followed by airway obstruction.
PREVALENCE OF AOP is related inversely to gestational age: • • Nearly 100% neonates with GA of <29 weeks or weight <100 g 54% of neonates with GA of 30 -31 weeks 15% of neonates with GA of 32 -33 weeks 7% of neonates with GA of 34 -35 weeks
3. CAUSES OF APNEA • Infection: - Sepsis, especially in the first day of life, and nosocomial infections and/or necrotizing enterocolitis (NEC) in the first weeks of life • Neurological: - Intraventricular hemorrhage, intracranial hemorrhage, neonatal seizures, perinatal asphyxia • Cardiovascular: - Impairment of oxygenation from congestive heart failure and pulmonary edema (PDA, coarctation, etc. ), or from shunting (cyanotic heart disease)
3. CAUSES OF APNEA • Pulmonary: - Impairment of oxygenation and ventilation from lung disease (surfactant deficiency disease, pneumonia, transient tachypnea of the newborn, meconium aspiration, etc. ) • Inborn errors of metabolism • Metabolic: - Hypocalcemia, hypoglycemia, hyponatremia or acidosis • Hematological: - Anemia
3. CAUSES OF APNEA • Gastrointestinal: - NEC or gastroesophageal reflux • Temperature Regulation: - Hypothermia or hyperthermia (think about transfer) • Drugs: - Prenatal exposure with transplacental transfer to the neonate of various drugs (narcotics, beta-blockers). Postnatal exposure to sedatives, hypnotics or narcotics.
4. INVESTIGATIONS FOR APNEA To exclude common causes of secondary apnea. Blood glucose Hematocrit Electrolytes, Septic screen, Blood culture Arterial blood gas Chest x-ray Abdominal x-ray, Head Ultrasound And other investigations depending on the history and physical examination
5. TREATMENT OF APNEA General measures: • Maintain airway, breathing and circulation (ABC) • Avoid vigorous suctioning of the oro-pharnyx (bulb suction) • Avoid oral feeds at least 24 hours. • Be cautious with fluctuations in temperature • Treatment of the underlying cause • Transfuse packed cells if hematocrit <30%
5. TREATMENT OF APNEA Specific measures: • Drugs including caffeine and/or aminophylline • Continuous positive airway pressure (CPAP) • Mechanical ventilation
6. EMERGENCY TREATMENT • The neonate should be checked for bradycardia, cyanosis and airway obstruction. • The neck should be positioned in slight extension; oro-pharnyx gently suctioned • Tactile stimulation should be given. • Most apneic spells respond to tactile stimulation.
6. EMERGENCY TREATMENT • Provide O 2 if hypoxia (maintain Sp. O 2 : 92 -95%) by head box or nasal cannula • If apnea persits and no response to tactile stimulation, ventilation BMV using 100% O 2 • If BMV fails to initiate spontaneous respiration, consider positive pressure ventilation.
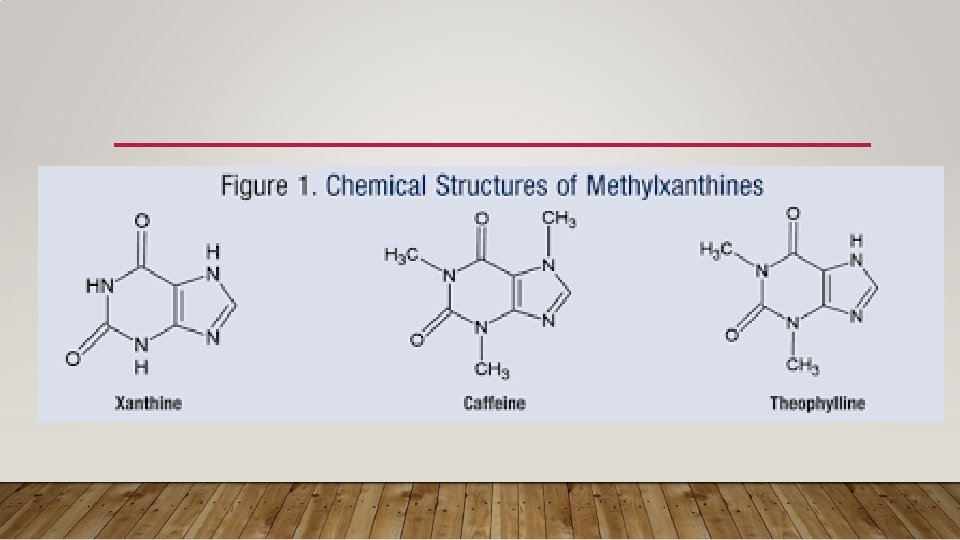
7. METHYLXANTHINES Keys determinants in choosing the appropriate drug: 1. Ease of administration, 2. Rapid response, 3. Minimal side effects, 4. Predictable plasma concentrations.
7. METHYLXANTHINES • Methylxanthines stimulate the central nervous system • They work by competitively antagonizing the adenosine receptor or increasing catecholamine release by modulating the flux of calcium. • They’ve been the mainstay of pharmacologic treatment of apnea for decades. • Adverse effects include tachycardia, emesis and jitteriness. • Both aminophylline and caffeine are used, but caffeine citrate is preferred because of its longer half-life, higher therapeutic index, and lack of need for druglevel monitoring.
8. COMPLICATIONS OF AOP • Spastic diplegia or quadriplegia • Bilateral retrolental fibroplasia resulting in significant visual impairment • Sensorineural deafness • Varying degrees of mental retardation.
9. SURVEILLANCE AOP • All newborns less than 34 weeks gestational age, or less than 1800 grams birth weight, should be monitored for both apnea and bradycardia. • Bradycardia by itself is often a sign of obstructive apnea. • No apnea alarm is sounded because the chest wall is moving even through air flow is absent. • Also reflex apnea can lead to bradycardia within 2 seconds of onset • Thus setting off the cardiac alarm 10 to 15 seconds ahead of the apnea alarm.
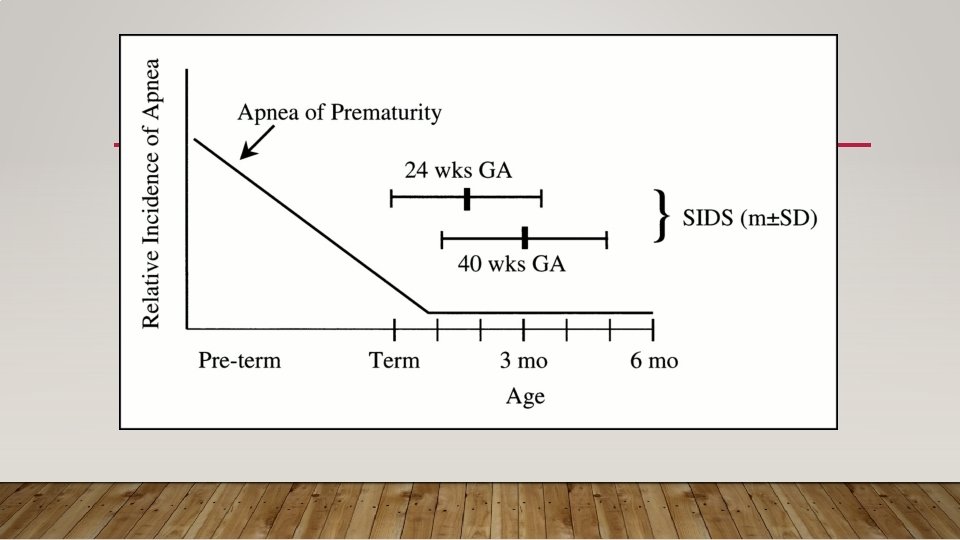
When AOP is well managed, luckily, it has no long term damage or is in any way related to sudden infant death syndrome (SIDS)
REFERENCES • Up. To. Date 2018 • Medscape/Apnea of Prematurity • Pediatrics. In. Review
THANK YOU ALL!!!!!!! Any question or comment?