Acute Confusional States Coma Introduction Definition of Consciousness



 phenomena because it represent a new")




 Headache: Head")
 General examination: - Meningismus: Meningitis, subarachnoid hemorrhage. - Skin rash: Meningococcal meningitis. -")
 Cranial nerves: - Papilledema: Hypertensive encephalopathy, intracranial mass. - Dilated pupils: Head trauma,")
 Motor: - Tremor: Withdrawal from ethanol or sedative drugs, sympathomimetic intoxication, thyrotoxicosis. -")
 Other: - Seizures: withdrawal from ethanol or sedative drugs, head trauma, hyperglycemia, hypoglycemia.")
Blood tests: - WBC: Meningitis, encephalitis, sepsis. -")
 Urine, gastric aspirate: - Drug screen: Drug intoxication. 3) Stool: - Occult blood:")
 C. S. F: - WBC, RBC: Meningitis, encephalitis, subarachnoid hemorrhage. - Gram's stain:")
 CT brain scan or MRI: Cerebral infarction, intracranial hemorrhage, head trauma, toxoplasmosis, herpes")


 - Metabolic: Drug overdosage (including alcohol) Hypoglycaemia D.")
 Structural: a. Diffuse: - Meningitis - Encephalitis - Other infections (e. g. cerebral")


 Is the airway clear? Check blood")
,")



 • • Metabolic acidosis, Diabetic ketoacidosis,")
, Cerebral abscess,")

 Every comatose patient should receive the following drugs immediately: - 50")
- Slides: 34
Acute Confusional States & Coma
Introduction • Definition of Consciousness: - Consciousness or conscious state or conscious self or conscious mind refers to a state of cerebral arousal which allows the brain to executes it’s functions of sensory perception of data input to it from the 5 common senses. - It refers to all perceptions, memories, feeling, ideas & fantasies …… that we currently appreciating. - It is non-spatial entity that has no direct location in space (spatial field) but has existence in temporal field. We can give it a location in space indirectly by link it to heir/him generating brain.
• “Brain - consciousness” relationship: ‒ Conscious mind is the product of brain, i. e. the brain is the generator of consciousness. ‒ Though the conscious mind is a spine of brain, but it is not just an epiphenomenon of brain physiology, i. e. not all it’s aspects can be reduced to physiology of brain. ‒ It is of dual nature containing elements which are merely reflections to brain activities & other elements which represent a pure psychic functions that represent a pure mental activities of consciousness not related to brain physiology, like anti-dating phenomenon. ‒ This mean that there is a bi-traffic way between the brain & the conscious mind. From material brain to consciousness (like energy to matter) as in sensory perception, & from consciousness to brain (like matter to energy) as in action of conscious self over the brain in voluntary movements & attention. ‒ In the usual conditions this mutual relation happen between conscious mind & it’s generating brain, not with other material entities.
‒ consciousness must contain such pure psychic (nonbrain) phenomena because it represent a new (completely new) level of organic evolution. ‒ If it involves just phenomena that represent reflections of the brain activities, this mean that it is a passive entity which mean that it is a non-adoptive character. This completely counter duct with laws of organic evolution, because from evolutionary point of view the consciousness has a survival (adoptive) value to the organism by allowing it to interact more efficiently with environment e. g. feeling pain from burn make you escape from fire. ‒ It represent merely a higher (the highest) level of organic evolution.
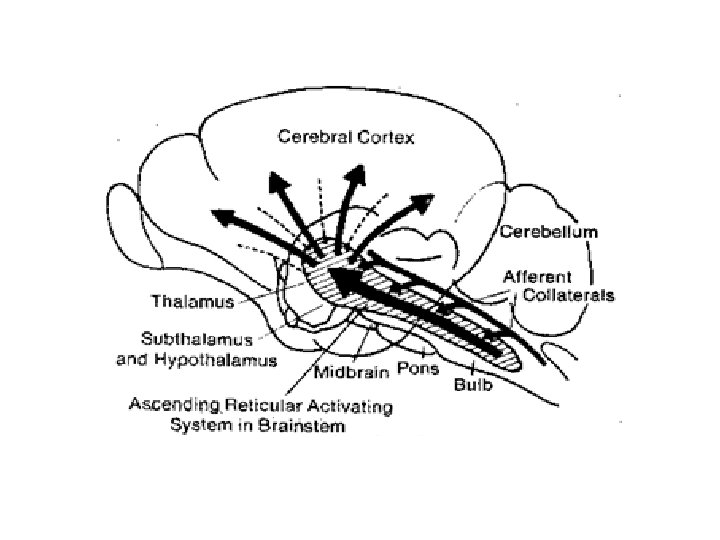
• Generation of conscious state depend on activity of a part from the reticular formation of brain called the ascending reticular activating system (A. R. A. S) of midbrain. • A. R. A. S terminated proximally in the non-specific thalamic nuclei (intra-laminary & midline thalamic nuclei) which project, in turn, non-specifically to the cerebral cortex. • Activity of this system act to generate a state of desynchronizations in cerebral cortex, which is necessary for execution of sensory perceptions & generation of consciousness.
What is the Nature of Consciousness? It is still unknown. It is an entity of unknown nature like time. Sigmund Freud said what mean: “study consciousness without tired yourself in the question of what is it’s nature, as for physicists who study the time & discover it’s laws without knowing exactly what is the time”. The question of “what is the nature of consciousness” is, as for the questions of what is the nature of time, remain a duty for future researches & discoveries.
Disturbances of Level of Consciousness • Normal level of consciousness: - Constant level of consciousness (no fluctuation = clear conscious stream) - Oriented in space, time & person - No hallucinations, no irritability • We have 2 major categories of disturb consciousness: 1) Hyperconsciousness: - Same of above but there is irritability. 2) Lowering level of consciousness: - Vary from: drowsiness, obtandation, confusion, delirium, stupor, semi coma, to coma. N. B: disturbances in level of consciousness result from disorders of or adverse effects on A. R. A. S of mid-brain.
Acute Confusion It is a state characterized by: 1. Disorientation in space & time, 2. Fluctuating level of consciousness & clouding of sensorium, 3. Acute onset & resent course. If hallucinations (usually visual) supper added to the above feature, the condition termed “delirium”.
Clinical Features Helpful in the Differential Diagnosis of Acute Confusional States: 1) Headache: Head trauma, meningitis, subarachnoid hemorrhage. 2) Vital signs: - Fever: Infectious meningitis, anticholinergic intoxication, withdrawal from ethanol or sedative drugs, sepsis. - Hypothermia: Intoxication with ethanol or sedative drugs, hepatic encephalopathy, hypoglycemia, hypothyroidism, sepsis. - Hypertension: Anticholinergic intoxication, withdrawal from ethanol or sedative drugs, hypertensive encephalopathy, subarachnoid hemorrhage, sympathomimetic intoxication. - Tachycardia: Anticholinergic intoxication, withdrawal from ethanol or sedative drugs, thyrotoxicosis, sepsis. - Bradycardia: Hypothyroidism. - Hyperventilation: Hepatic encephalopathy, hyperglycemia, sepsis. - Hypoventilation: Intoxication with ethanol or sedative drugs, opioid intoxication, pulmonary encephalopathy.
3) General examination: - Meningismus: Meningitis, subarachnoid hemorrhage. - Skin rash: Meningococcal meningitis. - Tetany: Hypocalcemia.
4) Cranial nerves: - Papilledema: Hypertensive encephalopathy, intracranial mass. - Dilated pupils: Head trauma, anticholinergic intoxication, withdrawal from ethanol or sedative drugs, sympathomimetic intoxication. - Constricted pupils: Opioid intoxication. - Nystagmus/ophthalmoplegia: Intoxication with ethanol, sedative drugs, or phencyclidine, vertebrobasilar ischemia, Wernicke encephalopathy.
5) Motor: - Tremor: Withdrawal from ethanol or sedative drugs, sympathomimetic intoxication, thyrotoxicosis. - Asterixis: Metabolic encephalopathy. - Hemiparesis: Cerebral infarction, head trauma, hyperglycemia, hypoglycemia.
5) Other: - Seizures: withdrawal from ethanol or sedative drugs, head trauma, hyperglycemia, hypoglycemia. - Ataxia: intoxication with ethanol or sedative drugs, Wernicke’s encephalopathy.
Laboratory Studies in Acute Confusional States: 1)Blood tests: - WBC: Meningitis, encephalitis, sepsis. - PT and PTT: Hepatic encephalopathy. - Arterial blood gas: Hepatic encephalopathy, pulmonary encephalopathy, uremia, sepsis. - Sodium: Hyponatremia. - Serum urea nitrogen and creatinine: Uremia - Glucose: Hyperglycemia, hypoglycemia. - Osmolality: Alcohol intoxication, hyperglycemia. - Liver function tests, ammonia: Hepatic encephalopathy, Reye syndrome. - Thyroid function test: Hyperthyroidism, hypothyroidism. - Calcium: Hypercalcemia, hypocalcemia. - Drug screen: Drug intoxications. - Cultures: Meningitis, sepsis. - FTA or MHA-TP: Syphilitic meningitis. - HIV antibody titer: AIDS and related disorders.
2) Urine, gastric aspirate: - Drug screen: Drug intoxication. 3) Stool: - Occult blood: Hepatic encephalopathy. 4) ECG: Anticholinergic or sympathomimetic intoxication (tachyarrhythmia), vascular disorders.
5) C. S. F: - WBC, RBC: Meningitis, encephalitis, subarachnoid hemorrhage. - Gram's stain: Bacterial meningitis. - AFB stain: Tuberculous meningitis. - India ink stain: Cryptococcal meningitis. - Cultures: Infectious meningitis. - Cytology: Leptomeningeal metastases. - Glutamine: Hepatic encephalopathy. - VDRL: Syphilitic meningitis. - Cryptococcal antigen: Cryptococcal meningitis. - Polymerase chain reaction: Bacterial meningitis, tuberculous meningitis, syphilitic meningitis, Lyme disease, viral meningitis and encephalitis, AIDS, leptomeningeal metastases.
6) CT brain scan or MRI: Cerebral infarction, intracranial hemorrhage, head trauma, toxoplasmosis, herpes simplex encephalitis, subarachnoid hemorrhage, intracranial tumor. 7) EEG: Complex partial seizures (epileptiform discharge over temporal or frontal lobes), herpes simplex encephalitis (periodic triphasic complexes over temporal or frontal lobes), hepatic encephalopathy (generalized triphasic waves), nonconvulsive seizures (epileptic discharges).
Treatment of Acute confusion This done by identifying the primary cause & correct it.
Coma & Stupor • Coma: It is a sleep like condition characterized by prolong loss of consciousness from which the patient can not be aroused by vigorous stimuli. • Stupor: It is a sleep like state characterized by prolong loss of consciousness from which the patient can be partially aroused for transient period of time by vigorous stimuli. It represent a less degree of disturb consciousness than coma.
Outline of causes of Coma A) - Metabolic: Drug overdosage (including alcohol) Hypoglycaemia D. M Renal failure Hepatic failure Hypothermia Hypothyroidism Cardiorespiratory failure Hypoxic encephalopathy
2) Structural: a. Diffuse: - Meningitis - Encephalitis - Other infections (e. g. cerebral malaria) - Subarachnoid hemorrhage - Epilepsy - Head injury - Hypertensive encephalopathy
b. Focal: * Supratentorial lesions: - Cerebral hemorrhage - Cerebral infarction with edema - Subdural hematoma - Extradural hematoma - Tumor - Cerebral abscess - Pituitary apoplexy
* Subtentorial lesions: - Cerebellar hemorrhage - Pontine hemorrhage - Brainstem infarction - Tumor - Cerebellar abscess - Secondary effects of transtentorial herniation of brain due to cerebral mass lesions
Immediate Assessment of Coma: * 7 questions: 1) Is the airway clear? Check blood gases to evaluate this issue. Intubate & give oxygen if there is airway compromisation. 2) Is the patient fitting? EEG/blood glucose. Give I. V glucose, oxygen & diazepam. 3) Are there sings of cranio-facial trauma? C. T scan & request neurosurgical opinion. 4) Is the neck broken? Use X-ray to verify this issue. Splint neck if exist. 5) Is there major hemorrhage? Maintain circulation. 6) Is there evidence of D. M? Send for blood/urine glucose. Treat appropriately. 7) Is there evidence of drug overdose or misuse? Check pupils/ventilation. Naloxone?
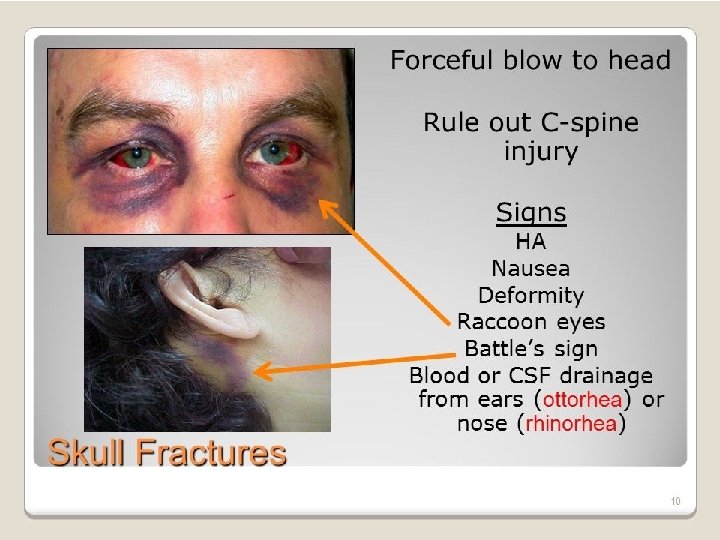
Basic Neurological Examination in Coma • Assess level of consciousness (use Glasgow coma scale), • Signs of head injury: local bruising (like raccoon eyes & Battle sign), fractures & penetrating wounds, bleeding from nose or ears, • Splint the neck: head injury may be associated with fracture of cervical spine, • If no neck injury (clinically & X-ray) check for neck stiffness, • Check resting pupillary size, & pupillary responses to light, • Ocular movements: spontaneous, following & to ‘doll’s head’ (should done if no voluntary response), • Limbs: posture, tone & movement, • Reflexes & plantar responses, • Fundi
Causes of Coma without Focal Neurological Signs, or Neck Stiffness: Metabolic coma: - Hypoglycaemia - Hyperglycaemia - Liver failure - Renal failure - Respiratory failure with CO 2 retention - Endocrine/electrolyte imbalance - Drug poisoning (consider gastric lavage)
Causes of Coma with Neck Stiffness: • • • SAH Meningitis Encephalitis Intracerebral hemorrhage Cerebral malaria N. B: Neck stiffness may be relatively unapparent in deeply comatose patients.
Coma with hyperventilation (& low Pa. CO 2) • • Metabolic acidosis, Diabetic ketoacidosis, Brainstem lesion, e. g. stroke, Raising intracranial pressure, Bacterial meningitis, Renal failure, Liver failure, Pneumonia complicating brain lesion.
Causes of Coma with Focal Neurological Signs: Epilepsy, Stroke, Encephalitis, SAH (occasional), Cerebral abscess, Bacterial meningitis with cortical infarction (occasional), • Cerebral venous sinus thrombosis. • • •
Essential Investigations in Coma • • • Cervical spine X-ray, CT head scan, Chest X-ray, X-ray of suspected fractures/bruised limbs, Blood for cross-matching, Complete blood picture, Drug screen, Electrolytes, blood sugar, renal & liver function tests, Blood gases & p. H L. P for C. S. F study (if there is suspicion of C. N. S infection or SAH or the cause of coma remain unknown). It should be proceeded by CT head scan to rule S. O. L
Very Important A) Every comatose patient should receive the following drugs immediately: - 50 cc of 50% hypertonic glucose I. V (possible hypoglycemia) - 100 mg thiamine I. V (since administration of dextrose alone may precipitate or worsen Wernicke’s encephalopathy in thiaminedeficient patients) - 0. 4 – 1. 2 mg naloxone I. V (possible opiate poisoning) B) Flumazenil 0. 2 – 0. 3 mg I. V, repeated once, then 0. 1 mg I. V dosing to max. of 1 mg), should only use in coma due to sedative-hypnotic drug intoxication & should not be included as standard treatment of coma of unknown cause, since in patient with some combined drug overdose with, e. g. cocaine or tricyclic agent in addition to a benzodiazepine, Flumazenil can precipitate status epilepticus.