Inflammation Inflammation The response of living vascularised tissues









 Attachment of opsonized particles to Fc & C 3 b receptors")


 and eliminate")








")
 Oxygen metabolites Nitric oxide")






 obstruction and")
 relatively short duration, lasting for minutes,")





 v↑ vascular permeability. v. Vasodilatation. v. Increase leukocytes adhesion.")
- Slides: 40
Inflammation
Inflammation The response of living vascularised tissues to injury 1 - Acute inflammation 2 - Chronic inflammation
Acute inflammation Early response of tissue to injury Vascular Non-specific Short duration
Components of acute inflammatory response Vascular 1. Transient vasoconstriction of arterioles : It disappears within 3 -5 seconds in mild injuries 2. Active vasodilatation of arterioles-Histamine-mediated result in (Hyperemia- increased blood in the area) 3 -Increased vascular permeability Histamine-mediated , result in (Increased fluid & high MW proteins pass through widened intercellular junctions)
- 4. Formation of fluid exudate, from circulation to the interstitial tissues. Fibrin-rich fluid - Contains plasma proteins including Ig, C’ and fibrinogen. - Helps combat the offending agent by diluting it, increase lymphatic flow and flooding the area with Ig+C’.
Mechanisms of inflammation
Pneumonia- exudation
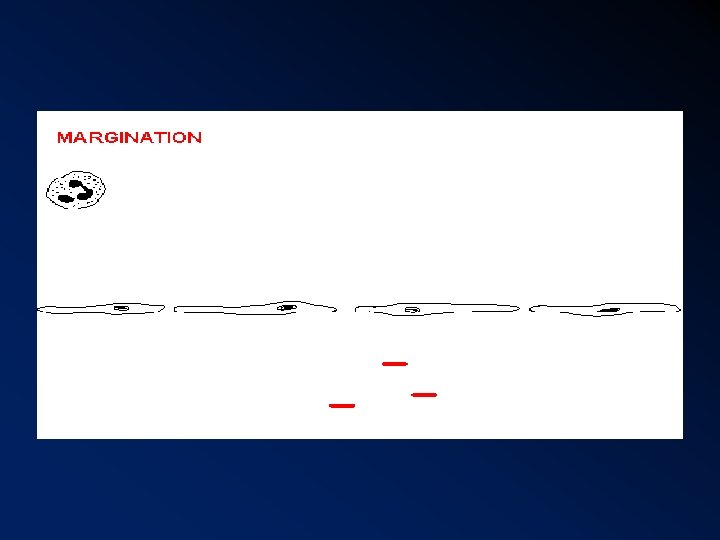
Cellular response A. types of cells involved 1 st 24 hours- neutrophils 24 48 hours – macrophages, lymphocytes, plasma cells. B. Margination of neutrophils Due to rouleaux formation of red cells and decreases in plasma. C. pavementing of neutrophils Marginated neutrophils adhere to endothelial surface.
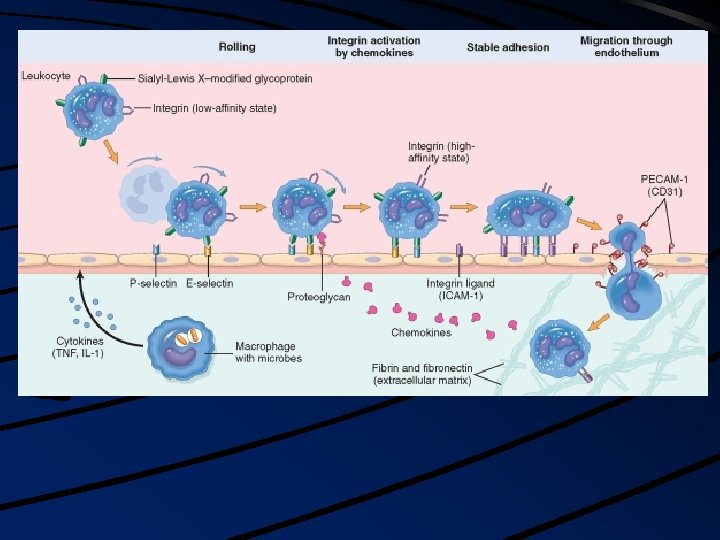
D. Emigration of neutrophils Neutrophils leave blood vessel through intercellular junction into interstitial tissue (3 -10 mins) E. Chemotactic factors C 5 a, leukotriene B 4, bacterial products Neutrophils have receptors for these factors F. Movement of other cells Macrophages and lymphocytes also mediated by lymphokines Passive entry of red cells.
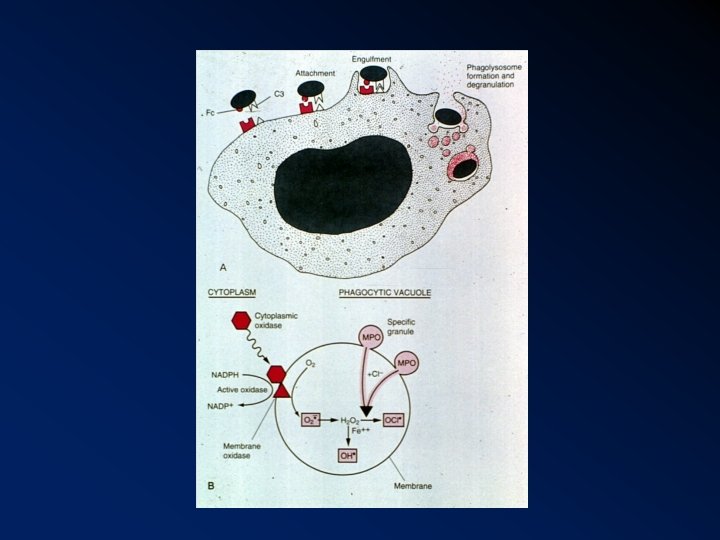
Phagocytosis: Involves: a) Attachment of opsonized particles to Fc & C 3 b receptors on the surface of leukocytes. b) Engulfment by pseudopods encirciling the phogocytosed particles, creating aphagosome. c) . Fusion of lysosomal granules with the phagosome, leading to degranulation. d) Types of bactericidal mechanisms: ( Killing and degradation bacteria. 1. O 2 - dependent mechanism O 2→superoxide 2. O 2 - independent mechanisms e. g lysozyme, lactoferrin
Defects in leukocyte function: ü ↑ susceptibility to infections. ü Genetic and acquired. Include: 1. Deficiency in circulating cells (neutropenia). 2. Defects in adherence. 3. Defects in migration and chemotaxis. 4. Defects in phagocytosis e. g. DM. 5. Defects in mitochondrial activity. 6. Mixed defects.
Components of acute inflammation Vascular changes Vasodilation: alterations in vessel caliber resulting in increased blood flow Increased vascular permeability: permit plasma proteins to leave the circulation Cellular events Emigration of the leukocytes from the microcirculation and accumulation in the focus of injury Principal leukocytes in acute inflammation are neutrophils (polymorphonuclear leukocytes).
Inflammation serves to destroy, dilute or isolate the injurious agent (microbes, toxins) and eliminate the necrotic cells and tissues.
The 5 cardinal signs of
Cardinal signs of acute inflammation Color—heat Rubor—redness Tumor—swelling Dolor—pain Functio laesa—loss of function
Redness/ Heat Increased rate and volume of blood flow into inflamed area Swelling Accumulation of exudate in the tissues Pain Accumulation of chemicals (prostaglandins) that stimulate nerve endings. Increased tissue tension
Redness
Swelling
Cardinal Signs of Inflammation
Mediators of acute inflammation Vasodilatation Histamine Prostaglandins Nitric oxide Increased vascular permeability Histamine Complements C 3 a, C 5 a Bradykinin Leukotrienes C 4, D 4, E 4 Platelet aggregating factor
Chemotaxis/ leucocyte activation Complement C 5 a Leucotriene B 4 Bacterial products Cytokines (IL-8) Fever Interlukins IL-1, IL-6 Tumour necrosis factor (TNF) prostaglandins
Pain Prostaglandins Bradykinin Tissue damage Lysosomal enzymes (neutrophil, macrophages) Oxygen metabolites Nitric oxide
Edema Excess of fluid in the interstitial space. Either exudates or transudate. Exudates Inflammatory extravascular fluid with high protein content, cellular debris, SG 1. 012 Transudate Fluid with low protein content. SG< 1. 012 Pus Inflammatory exudate rich in neutrophils and debris
Types of inflammatory exudate Serous ; Fluid exudation. Burns Fibrinous ; Excess fibrin formation. Bacterial infections Membranous / pseudo-membranous. Necrotic exudates adherent to mucosal surface Diphtheria, antibiotic-assoc. colitis Haemorrhagic ; Marked necrosis and haemorrhage. Virulent organisms
Catarrhal ; Excess mucus, common cold Suppurative ; Marked neutrophils response with pus. Pyogenic infections Allergic : Marked edema. urticaria
Cellulitis Spreading inflammation with tissue necrosis Nitric oxide Soluble free radical gas Produced by Endothelial cells Macrophages
Outcome / Sequelae of acute inflammation Resolution : Return to normal structure and function Healing by fibrosis/ later fibrous scar Suppuration / abscess Chronic inflammation : Persistence of acute inflammation converts response to a chronic type
Effects of acute inflammation 1. 2. 3. 4. 5. 6. Beneficial effects Dilution of toxin Entry of antibodies Transport of drugs Fibrin formation Delivery of nutrients & oxygen Stimulation of immune response
Harmful effects 1. Enzyme digestion of normal tissues 2. Swelling- causing (respiratory) obstruction and raised (intracranial) pressure 3. Inappropriate inflammatory response eg. Type 1 hypersensitivity reaction
Acute inflammation rapid in onset (seconds or minutes) relatively short duration, lasting for minutes, several hours, or a few days its main characteristics: the exudation of fluid and plasma proteins (edema) the emigration of leukocytes, predominantly neutrophils. Chronic inflammation is of longer duration associated histologically with the presence of lymphocytes and macrophages, the proliferation of blood vessels, fibrosis, and tissue necrosis. Less uniform.
Chemical mediators: 1. Histamine & serotonin: found in: v Mast cells. v Basophils v Platelets. Action : 1. Vasodilatation 2. ↑ vascular permeability. Release from mast cells is caused by: 1. Physical agents. 2. Immunologic Ig. E reactoin. 3. C 3 a & C 5 a anaphylatoxin.
4. Interleukin-1. 5. Other histamine releasing factors. Release from platelets is stimulated by: a. Contact with collagen. b. Thrombin. c. ADP. d. Antigen- antibody complexes. e. Platelets activating factor (PAF). 2. Complement system: Activation of complement system occurs via : i. The classic pathway, initiated by antigen-antibody complexes.
ii. Alternate complement pathway, activated by: Ø Endotoxin Ø Complex polysaccharides Ø Aggregated globulins. Coplement components with inflammatory activity include: 1. C 3 a, which increase vascular permeability. 2. C 5 a, “ “ “ and leukocytes chemotaxis. 3. C 3 b, C 3 bi the opsonins important in phagocytosis.
4. C 5 b- 9 the membrane attack complex that a. Lyses cells b. Stimulate arachidonic acid metabolism. c. Production of reactive O 2 metabolities by leukocytes. 3. Kinin system: 1. bradykinin→↑ vasopermeability. 2. Kallikrein has chemotatic activity & causes neutrophil aggregation.
4. Clotting system: Fibrinogen → fibrinopeptides. 1. ↑vascular permeability. 2. Chemotatic. 5. Arachidonic acid metabolities: The inflammatory prostaglandins & leukotreines include: 1) Prostacyclin: PGI 2 &PGE 2→ vasoconstriction. 2) Leukotreines, C 4, D 4, & E 4, ↑permeability & vasoconstriction. 3) Thromboxane A 2: → vasoconstriction. 4) Leukotreine B 4 → chemotaxis.
6. Platelet activating factor (PAF) v↑ vascular permeability. v. Vasodilatation. v. Increase leukocytes adhesion. v. Leukocytes chemotaxis. 7. Cytokines: - Polypeptides. - Released by macrophages and lymphocytes. - Example, IL-1, TNF, IL-8