Pathophysiology L 4 Inflammation Prof Fakhir AlAni fakeralani














")
 Vaso-dilation Slowing of the circulation Outpouring of albumin")


 & parenchymal")









")










- Slides: 41
Patho-physiology L 4 Inflammation Prof. Fakhir Al-Ani fakeralani 2000@yahoo. com
Inflammation It is a protective response of the body against injury. Include reaction of: The living tissue & micro-circulation to a pathogenic insult. It acts as defense & healing mechanisms to the site of injury. It is “A dynamic response of vascularised tissue to injury. ”
Etiologies Any stress = Injurious agent Ø Microbial infections: Bacterial, Viral, Fungal, etc. Ø Physical agents: Burns & radiation, Trauma like cuts. Ø Chemicals: Drugs, Toxins, Caustic subs. Or strong acid. Ø Immunologic reactions: Rheumatoid arthritis.
Injury Acute inflammation Abscess Chronic inflammation Resolution Repair
Inflammatory response Pathologically: - Vasoconstriction - Followed by vasodilatation These will cause: - Stasis - Hyperemia - Accumulation of leukocytes, - Exudation of fluid - Deposition of fibrin.
Mechanism: - How Does It Occur? Stimulus Tissue injury Release of Chemical mediators from the B. plasma & some cells. Induces vascular & cellular responses of inflammation
Chemical Mediators: Chemical subs. synthesized or released To mediate changes in inflammation. - Histamine: - by: -basophils & mast cells Cause Vasodilatation. - Prostaglandins: –by: -mast cell & Tissue Cause Pain & Fever. - Bradykinin: - by: - WBC & Tissue - Causes pain. - Leukotrienes: - Causes Pain & swelling
Chemical Mediators: Complement Chemotaxis. Opsonization: Coats bacterial surface; enhances phagocytosis & lyses bacteria Interferon Proteins that are released by helper T’s & kill viruses
Cardinal Signs of Inflammation Redness : Hyperaemia. Warm : Hyperaemia. Pain : Nerve, Chemical mediators. Swelling : Exudation Loss of Function: Pain
Type of inflammation According to the time: - Acute inflammation: < 48 hours - Chronic inflammation: > 48 hours (weeks, mon, years) According to the Cell type: - Acute inflammation: Neutrophils - Chronic inflammation: - Mononuclear cells (Macrophages, Lymphocytes, Plasma cells).
Type of inflammation
Pathogenesis: The inflammatory response is : 1. Release of chemical mediators : 2. Increased B. flow (redness & warmth). 3. Increased vascular permeability (swelling & Leukocytic Infiltration Also there is: - Loss of function, - Pain
Mechanism of Inflammation 1. Vaso dilatation 2. Exudation - Edema 3. Emigration of cells 4. Chemotaxis
1. Vaso dilatation Vascular dilation: - Blood flow: Erythema Warmth area - Permeability (1) Extravasation of fluid. (2) Deposition of plasma Pr. (edema). (3) Leukocyte emigration at the site of injury.
Changes in vascular flow (hemodynamic changes) Vaso-dilation Slowing of the circulation Outpouring of albumin rich fluid into the extravascular tissues results in the conc. of RBCs in small vessels & B. viscosity. Leukocyte margination Neutrophi become oriented at the periphery of vessels & start to stick.
Severity of injury & rapidity of inflammation Minor damage Severe damage 15 -30 minutes a few minutes
Transudate Versus Exodate Edema: Excess of fluid in the interstitial tissue Fluid could be: - Transudate : - An ultrafiltrate of B. plasma Low. Protein / Normal permeability - Exudate: - A filtrate of B. plasma mixed with inflammatory cells & cellular debris. High Protein/ Permeability Lymphatics are responsible for draining edema
Pus A purulent exudate: An inflammatory exudate rich in leukocytes (mostly neutrophils) & parenchymal cell debris.
Leukocyte exudation Divided into 4 steps 1. Margination, rolling, & adhesion to endothelium 2. Diapedesis (migration across the endothelium) 3. Chemotactic stimuli from the source of tissue injury. 4. Phagocytosis
Leukocyte exudation Steroids, leukocyte adhesion deficiency Diabedesis Chemo- taxis
Phagocytosis Steps of phagocytosis: - Recognition & attachment - Engulfment - Killing
Digestion of bacteria - Enzymes killing the bacteria: Hydrolytic enzyme. Peroxidase enzyme. -Digestive enzymes. Defect in these enzymes will cause: Chronic granulomatous disease (CGD)
Types of acute inflammation According to Morphology 1. Exudative or catarrhal Inflammation: Excess fluid = TB lung. 2. Fibrinous Excess of fibrin = Pneumonia 3. Membranous Fibrino-necrotic inflammation 4. Suppuration/Purulent Bacterial - neutrophils
4. Serous Excess clear fluid – Heart, lung 5. Allergic inflammation 6. Haemorrhagic B. V. damage - anthrax. 7. Necrotising inflammation.
Inflammation Outcome Fibrosis/Scar Resolution Injury Acute Inflammation Fungus Virus Cancers T. B. etc. Abscess Ulcer Fistula Chronic Inflammation Sinus
Outcome of Acute inflammation 1. Resolution--tissue goes back to normal 2. Chronic inflammation 3. Abscess formation 4. Repair--healing by scarring or fibrosis
Abscess formation: - It occurs in suppurative inflammation - It is a localized collection of pus (Dead tissue, Bacteria, WBCs) - It may occurs in an acute or chronic infection. - It is associated with tissue destruction, & swelling.
Abscess formation: Site: - Skin, subcutaneous tissue. - Internal organs (Brain, lung, liver, kidney) Pathogenesis: The necrotic tissue is surrounded by pyogenic membrane. The membrane is formed by fibrin & help in localize the infection.
Carbuncle - It is an extensive form of abscess in which pus is present in multiple loci open at the surface by sinuses. - Occur in the back of the neck & the scalp.
Furuncle or boil - It is a small abscess related to hair follicles sebaceous glands, could be multiple furunclosis. or
Cellulitis - Acute diffuse suppurative inflammation caused by streptococci. Streptococci secrete: Hyaluronidase & Streptokinase enzymes They dissolve the ground substances &facilitate the spread of infection. - Sites: - Areolar tissue; orbit, pelvis, … - Lax subcutaneous tissue
Healing There are 3 ways of healing depending on: - The tissue involved. - The degree of injury 1. Resolution - Damaged cells recover in short time - Ex = mild sunburn
Healing 2. Regeneration - Damaged cells replaced by identical cells via mitosis - Occurs only in epithelia & C. T. 3. Scar formation - Damaged tissue replaced by regeneration & scar formation. - Occurs in complex organ. - Due to highly vascular C. T.
Healing by Primary or Secondary intention Depend weather edges of lesion can be brought together: - Primary: Intention gives small scar formation - Secondary: Intention gives large scar formation Heals via granulation tissue
Burns Ø First degree burns - Superficial partial-thickness - Involves just epidermis - Get redness but no blistering - May peel in 1 -3 days without scarring Ø Second degree burns - Deep partial-thickness - Involves epidermis & dermis - Get redness & blistering - Can get scarring Ø Third degree burns - Full-thickness - Involves all 3 layers & involve underlying tissue - Get no pain
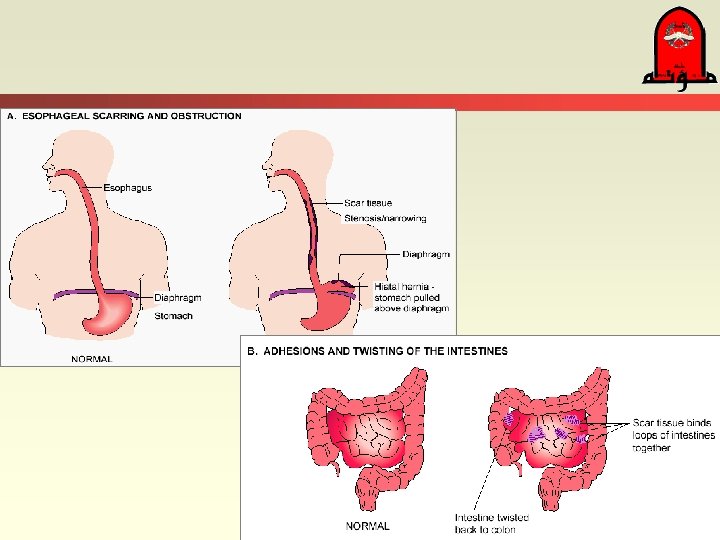
Complications of healing Healing with large scar formation: - lead to: – Contractures – Loss of function – & obstructions – Can lead to stenosis – Ulceration.
Factors delaying healing Old age Presence of foreign material Poor blood supply Poor nutrition Complications (bleeding, hematoma, excessive mobility