UNIT II Respiratory system Respiratory system Asthma Chronic


 • Clinical terms for a group of pathological conditions")






")








- Slides: 22
UNIT II Respiratory system
• Respiratory system: – Asthma – Chronic obstructive airways diseases
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) • Clinical terms for a group of pathological conditions in which – chronic, partial or complete, obstruction to the airflow – at any level from trachea to the smallest airways – resulting in functional disability of the lungs i. e. they are diffuse lung diseases • The following 4 entities are included in COPD: i. iii. iv. Chronic bronchitis Emphysema Bronchial asthma Bronchiectasis
CHRONIC BRONCHITIS • Persistent cough with expectoration for at least three months of the year for two or more consecutive years • The condition is more common in middle-aged males than females • Quite frequently, chronic bronchitis is associated with emphysema
ETIOPATHOGENESIS 1. 2. 3. 4. 5. Cigarette smoking Atmospheric pollution Occupation, Infection, Familial and genetic factors 1. Smoking. 4 to 10 times higher proneness, act on lungs: i. impairs ciliary movement ii. inhibits the function of alveolar macrophages iii. hypertrophy and hyperplasia of mucus secreting glands iv. causes considerable obstruction of small airways v. stimulates vagus and causes bronchoconstriction
2. Atmospheric pollution. industrialised urban areas sulfur dioxide, nitrogen dioxide, particulate dust and toxic fumes. 2. Occupation. cotton mills (byssinosis), plastic factories etc. - exposed to various organic or inorganic dusts 3. Infection. Bacterial, viral and mycoplasmal infections do not initiate chronic bronchitis but usually occur secondary to bronchitis. Cigarette smoke, predisposes to infection 4. Familial and genetic factors. familial tendency and genetic predisposition
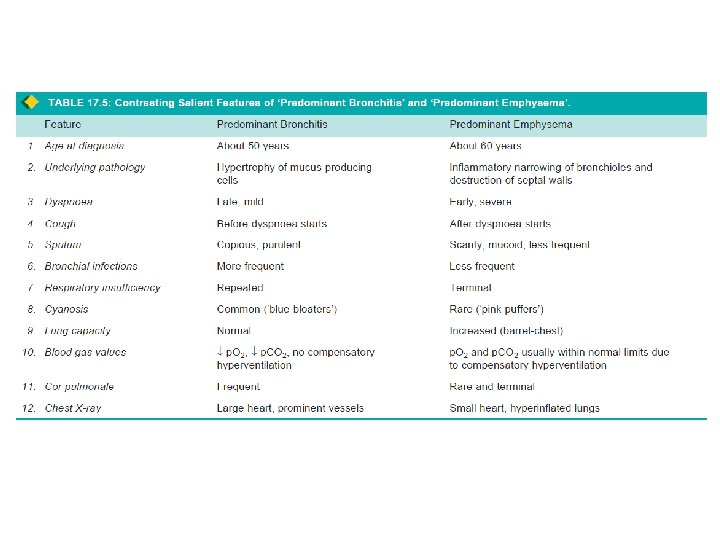
CLINICAL FEATURES • Considerable overlap of clinical features of chronic bronchitis and pulmonary emphysema (discussed below) as quite often the two coexist. • Contrasting features of ‘predominant emphysema’ and ‘predominant bronchitis’ are presented in Table 17. 5. • Important features of ‘predominant bronchitis’ are as under: 1. Persistent cough with copious expectoration of long duration 2. Recurrent respiratory infections are common 3. Dyspnoea is generally not prominent at rest but is more on exertion 4. cyanosis and oedema 5. Features of right heart failure (cor pulmonale) 6. Chest X-ray shows enlarged heart with prominent vessels
EMPHYSEMA • combination of – permanent dilatation of air spaces distal to terminal bronchioles and – destruction of the walls of dilated air spaces • Emphysema is defined morphologically, while chronic bronchitis is defined clinically. – two conditions coexist frequently and – show considerable overlap -clinical features, • it is usual to label patients as ‘predominant emphysema’ and ‘predominant bronchitis’
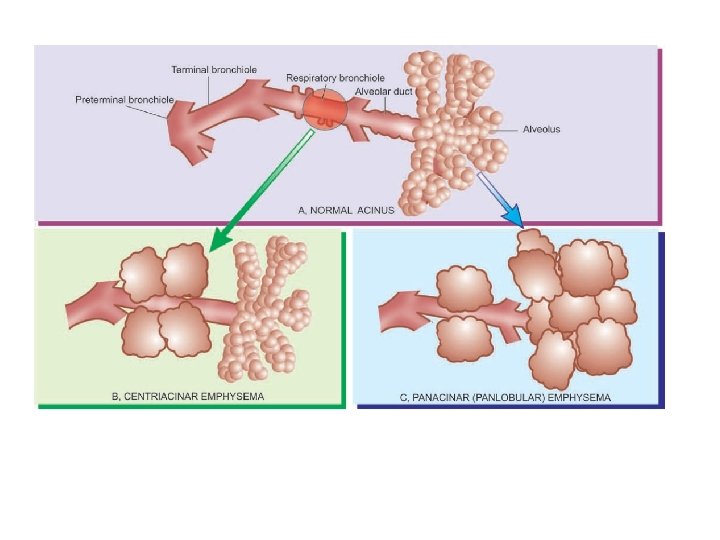
CLASSIFICATION • A lobule is composed of about 5 acini distal to a terminal bronchiole • An acinus consists of 3 to 5 generations of respiratory bronchioles and a variable number of alveolar ducts and alveolar sacs • pulmonary emphysema is classified according to the portion of the acinus involved (WHO definition), into 5 types: – Centriacinar, – Panacinar (Panlobular), – Para-septal (Distal Acinar), – Irregular (Para-cicatricial) – Mixed (Unclassified) • A number of other similar conditions are examples of ‘overinflation’
An acinus consists of 3 parts: • 1. Several (usually 3 to 5 generations) respiratory bronchioles originate from a terminal bronchiole • 2. Each respiratory bronchiole divides into several alveolar ducts. • 3. Each alveolar duct opens into many alveolar sacs (alveoli) which are blind ends of the respiratory passages.
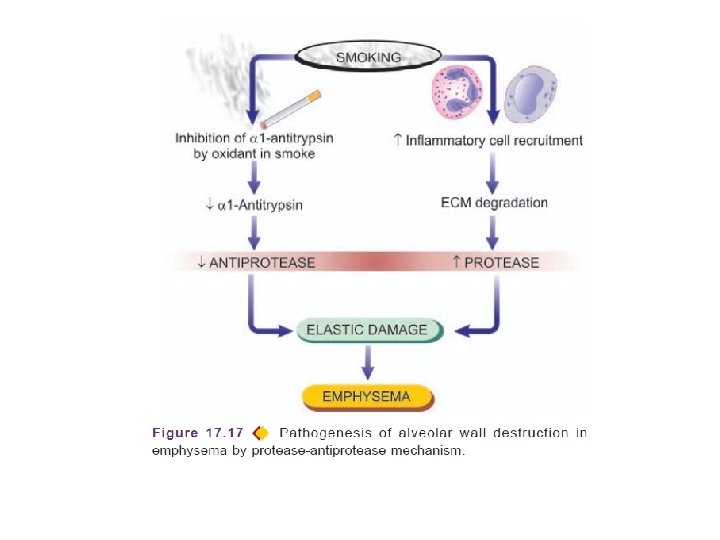
• Mechanism of alveolar wall destruction in emphysema by elastolytic action is due to imbalance between proteases (chiefly elastase) and anti-proteases (chiefly anti-elastase): • By decreased anti-elastase activity i. e. deficiency of α-1 antitrypsin. • By increased activity of elastase i. e. increased neutrophilic infiltration in lungs causing excessive neutrophil elastase. • Smoking promotes emphysema by both decreasing amount of antielastase as well as by increasing elastolytic protease in lungs. These are as under: • 1. Oxidant in cigarette smoke has inhibitory influence on α-1 antitrypsin, thus lowering the level of anti-elastase activity. • 2. Smokers have up to ten times more phagocytes and neutrophils in their lungs than nonsmokers; thus they have very high elastase activity.
CLINICAL FEATURES • Clinical features develops after about one-third of the pulmonary parenchyma is damaged- occurs most severely in panacinar emphysema • Increasing severe exertional dyspnoea • Cough occurs late after dyspnoea • Respiratory infections • Tachypnoea • Weight loss is common • Features of right heart failure (cor pulmonale) and hypercapneic respiratory failure are the usual terminal events • Chest X-ray shows small heart with hyperinflated lungs
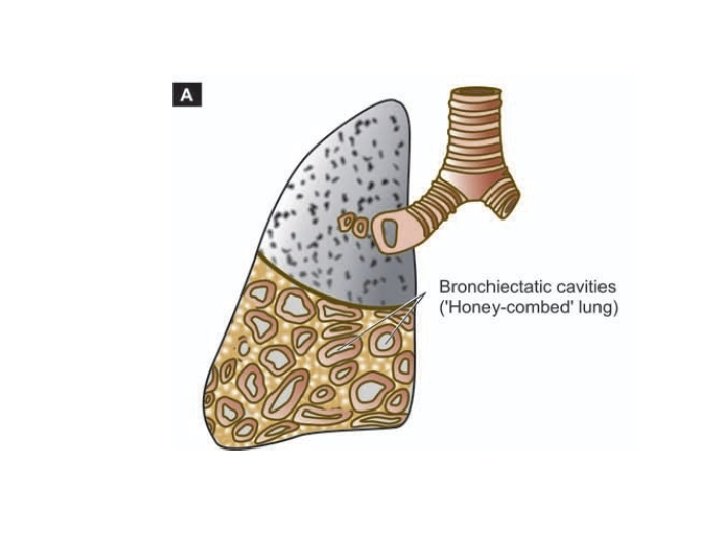
BRONCHIECTASIS • abnormal and irreversible dilatation of the bronchi and bronchioles (greater than 2 mm in diameter) developing secondary to inflammatory weakening of the bronchial walls • characteristic clinical manifestation - persistent cough with expectoration of copious amounts of foulsmelling, purulent sputum ETIOPATHOGENESIS • origin of inflammatory destructive process of bronchial walls- always result of two basic mechanisms: – endobronchial obstruction – infection
• Endobronchial obstruction by foreign body, neoplastic growth or enlarged lymph nodes causes resorption of air distal to obstruction with consequent – atelectasis (Collapse) and retention of secretions. • Infection may be secondary to local obstruction or infection may be a primary event - developing in suppurative necrotising pneumonia • 2 mechanisms—endobronchial obstruction, infection, are seen in a number of clinical settings as under: 1. Hereditary and congenital factors. Several hereditary and congenital factors may result secondarily in diffuse bronchiectasis: i. Congenital bronchiectasis caused by developmental defect of the bronchial system. ii. Cystic fibrosis, a generalised defect of exocrine gland secretions, results in obstruction, infection and bronchiectasis
2. Obstruction • Post-obstructive bronchiectasis, usually confined to one part of bronchial system • causes of endobronchial obstruction include – foreign bodies, – endobronchial tumours, – compression by enlarged lymph nodes and – post-inflammatory scarring (e. g. in healed tuberculosis)
3. As secondary complication. • Necrotising pneumonias- develop bronchiectasis as a complication – staphylococcal suppurative pneumonia – tuberculosis
Clinical symptoms • Chronic cough with foul smelling sputum production, haemoptysis and recurrent pneumonia, Sinusitis • Late complications - cases uncontrolled for years include development of clubbing of the fingers, metastatic abscesses (often to the brain), amyloidosis and cor pulmonale (Enlarge right heart due to lungs disease)
• Reference: Robbins, Basic Pathology by Elsevier