Treatment of severe acute malnutrition Experience from developmental







")


 •")

")










- Slides: 26
Treatment of severe acute malnutrition Experience from developmental context Jimma, Ethiopia Tsinuel Girma Asst professor of Pediatrics and Child Health Jimma University Mar 2008 (2000)
Child health indicators
Current U 5 MR trend Vs MDG trend
500, 000 under-5 dying each year Ranking 6 th in the world 72 % preventable f Other, 2% Measles, 4% AIDS, 1% Neonatal, 25% Diarrhea, 20% Malnutrition 57% HIV/AIDS 11% Malaria, 20% Pneumonia, 28%
Nutritional Status of Children Under Age Five
Key interventions selected for targeted condition NATIONAL STRATEGY FOR CHILD SURVIVAL IN ETHIOPIA , 2005 Malnutrition Prevention/promotion Breast feeding Complementary feeding Nutrition advice and supplementation Vitamin A supplementation PMTCT Measles vaccination Family Planning Clinical care Management of severe acute malnutrition Vitamin A Zinc Nutrition advice
In-patient treatment- hospital based • Opened as part of pediatric in-patient service (Feb 2004) • Maximum capacity of 30 patients • Staff : Feeders, nurses , interns , residents and consultants • Implementation of national protocol • Open 24 hrs
Achievements
Disciplined treatment, improved practicum set-up, new outlook about treating SAM and interest in nutrition related research
• More than 1350 patients treated so far most with co-morbidities (TB/HIV) • Death Rate < 6% • ARWG ~ 15 g/kg/d • ALOS 4 weeks
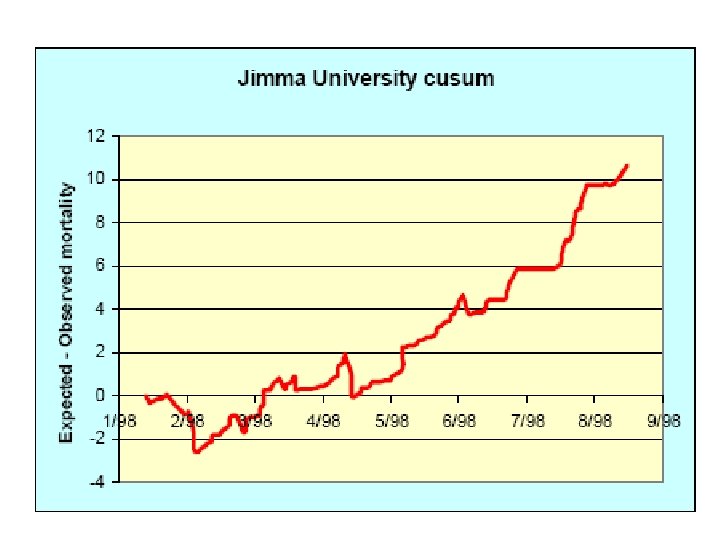
Observed and expected deaths from Jimma TFU using Prudhon Index
Out- Patient Treatment • • Context In 5 Health centers using RUTF (Dec 2005) Community mobilization and screening MOH is primarily responsible UNICEF provides RUTF and antibiotics Concern – Ethiopia: training Jimma University- Department of Pediatrics and Child Health
Performance Post-training follow –up, after 2 months in nine HCs showed • Implementation within 34 days (20 -58) • Enthusiastic health workers • Good acceptance by mothers and caregivers (also demonstrated in another study) But • Poor adherence to protocol ( one in five) • Poor medical recording • No proper evaluation of appetite – (field tested )
Types of malnutrition on admission n=324, four health centers
Treatment outcome
Outcome • RWG for recovered children was 6. 0 g/ kg/d and no difference between types of malnutrition • RWG for defaulters < 5 g/kg/d • Length of stay for all recovered children was 36. 0 and 39. 0 days, respectively.
different outcome between HCs but not on the type of malnutrition
Malnutrition and HIV/AIDS • Variable according to implementing agency so NO harmonized and standard care • Screening for SAM and treatment in adults is practically absent in most programs • Planned RCT in Jimma on supplementary feeding for patients on HAART
Challenges • • Staff turnover Supply breaks Sharing/ selling of RUFT Poor recording Protocol breach High defaulter rate Payment for drugs
Conclusion • Appropriate treatment of SAM and integration to routine health care delivery can save many lives • There is favorable environment: Interest in health service managers at different level, motivation of health workers and mothers by the treatment outcome • Quality of care has to be improved through constant supportive supervision, in-service training and strengthening pre-service training as long term solution
Conclusion … • Develop local expertise by working closely with higher learning institutions which is crucial for sustainability of new initiatives, research and development • There is an urgent need for more operational researches