Respiratory Insufficiency Sleep Apnoe Hypopnoe Syndrome SAHS Janos
 Janos Varga MD, Ph. D National Koranyi")
 - chronic")
 = (PB-47) x FIO 2 – 1. 2")

 time: 0. 75 s Equilibration: 0. 25")
, heart (ASD, VSD, Eisenmenger-sy) • Functional: V/Q=0;")


 Pulmonary vascular Heart failure")




 • One or more risk")
 in global respiratory insufficiency - Bi. PAP")
 • Dg: apnoe >5/h , >30/sleep period, SAT decrease: minimum")
 • Obstructive • Mixed Risk factors: -")


 • • • EEG EOG EMG EKG ABG, pulzoximetry Detection")


- Slides: 32
Respiratory Insufficiency Sleep Apnoe Hypopnoe Syndrome (SAHS) Janos Varga MD, Ph. D National Koranyi Institue for TB and Pulmonology Courtesy of Prof Attila Somfay MD, Ph. D
Classification of respiratory insufficiency 1. Progression in time – acute (p. H!) - chronic 2. Pathophysiology - type I (hypoxemia=Pa. O 2<60 Hgmm) - type II (hypoxemia + hypercapnia=Pa. CO 2>50 Hgmm) 3. Pathomechanism - V/Q mismatch - hypoventilation - limited diffusion - right-left shunt 4. Etiology - airway - lung parenchyma - lung vasculature - chest wall and pleura - neuromuscular
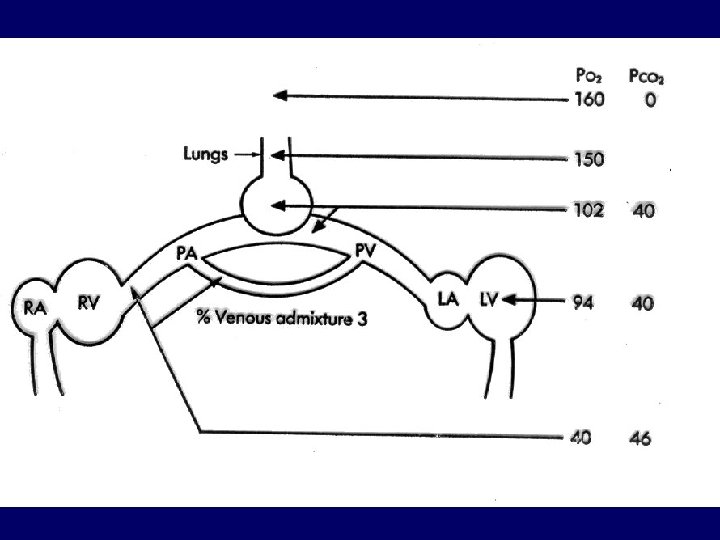
Alveolar gas equation: PA (mm. Hg) = (PB-47) x FIO 2 – 1. 2 x Pa. CO 2 102 = 150 - 48
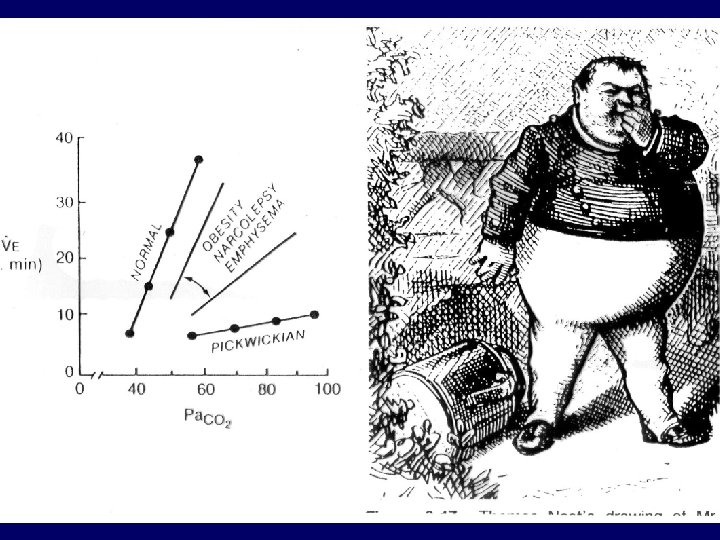
The causes of hypoventilation Site of abnormality Central Brain stem Spinal cord Peripheral nerves Neuromusc. Junction Upper airway Chest wall Respiratory muscles Disease Primary hypoventilation sy, barbiturat, opiat Encephalitis, haemorrh. , trauma Cervical trauma, poliomyelitis Guillain-Barré-sy, bilat. n. phrenicus paresis Myasthenia gravis Trachea stenosis Kyphoscoliosis, trauma Muscular dystrophies
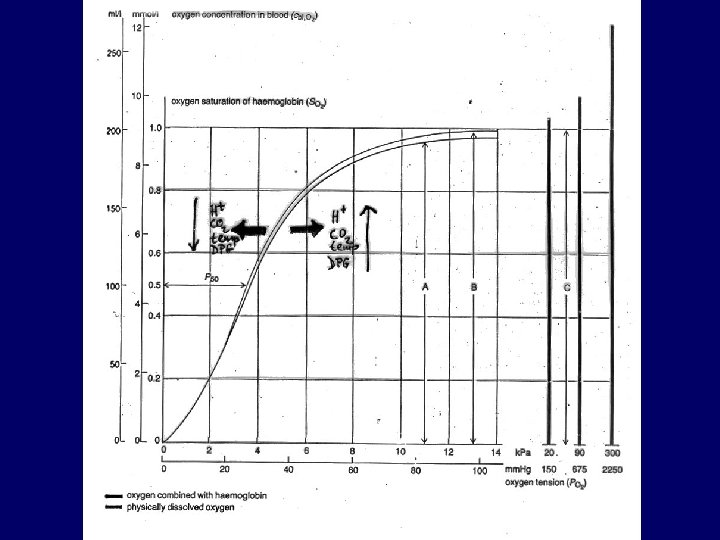
Diminished diffusion • • • Transit (contact) time: 0. 75 s Equilibration: 0. 25 s Exercise + diminished diffusion: Pa. O 2<60 Hgmm Pa. CO 2 : no change or decreases Causes: alveolitis fibrotisans, sarcoidosis, pneumoconiosis, connective tissue diseases, drugs, irradiation, alveolar cell cc, Goodpasture-sy, CHF
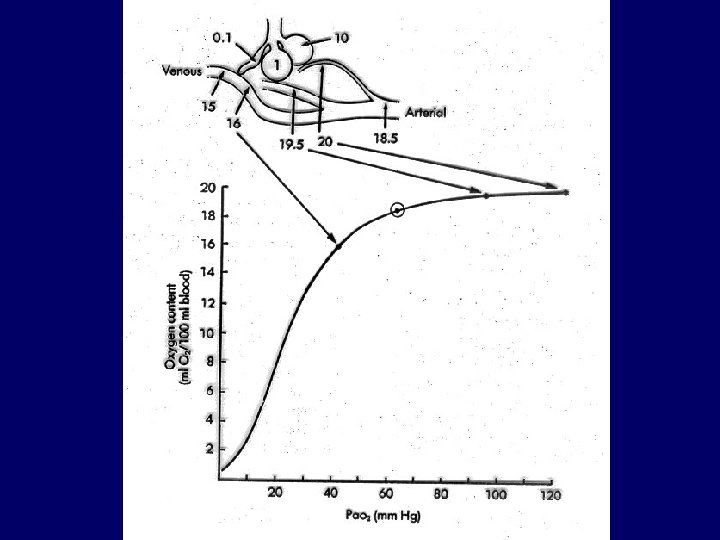
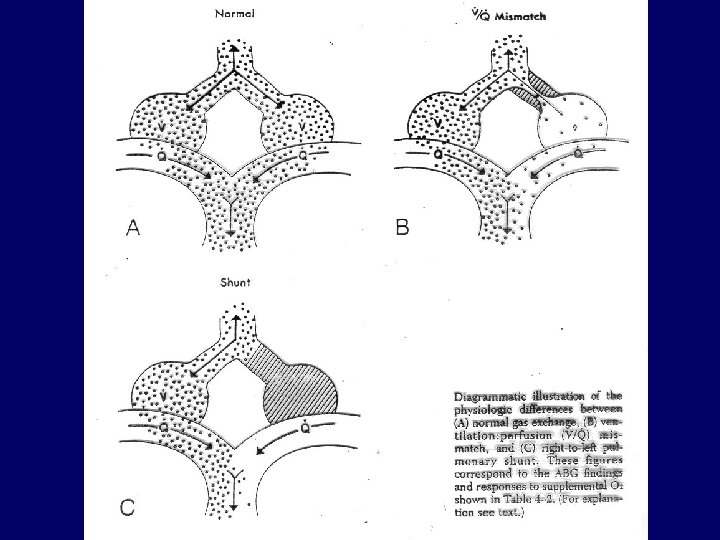
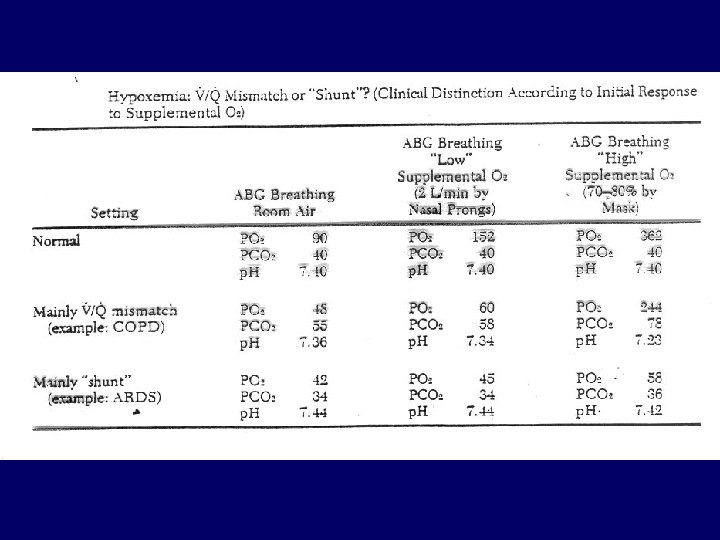
Right-left shunt • Anatomic: lung (a-v malformation), heart (ASD, VSD, Eisenmenger-sy) • Functional: V/Q=0; ARDS, atelectasia, oedema, haemorrhagia • Hypercapnia: no or rarely • Hypoxemia: cannot be corrected by 100% O 2
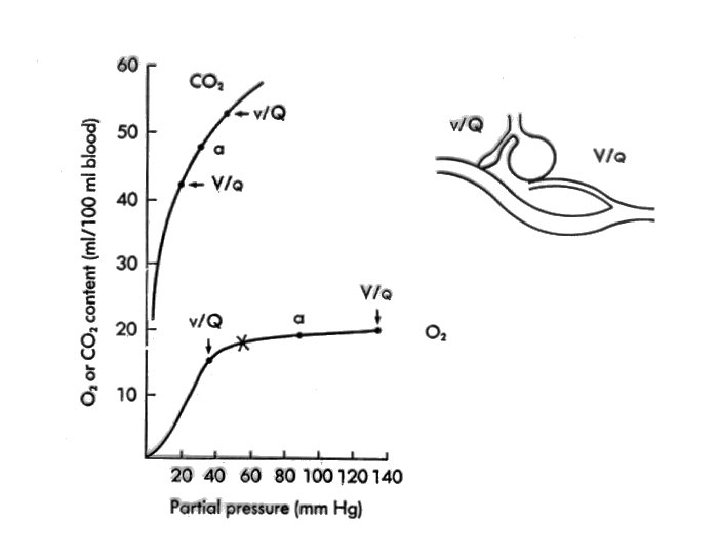
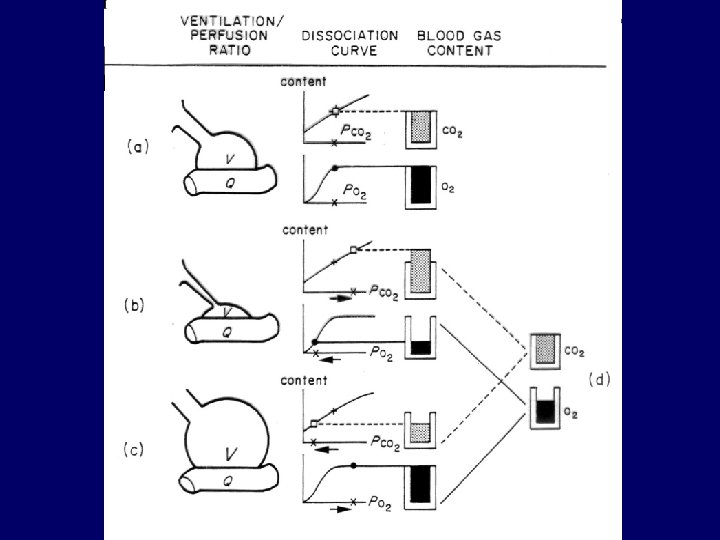
Ventilation-perfusion mismatch • “Functional shunt”, most frequent cause of hypoxemy • COPD, ILD, pulmonary embolism • Regional differences in airway resistance and lung compliance • Hypercapnia: only in severe cases (blue bloater) • Hypoxemia: correctable with small increase in FIO 2
Symptoms of hypoxemia és hypercapnia HYPOXEMIA Cyanosis Tachycardia Hypertension Headache Agitation Dezorientation Loss of consciousness Fibrillation, bradycardia Convulsions, retina bleeding Brain damage HYPERCAPNIA Warm, wet skin Tachycardia Hypertension Headache myosis, papilla oedema Agitation Dezorientation, sleepiness Tremor Pathologic reflexes Loss of consciousness Coma
Diseases leading to resp. insuff. Airway Lung parenchyma Hyperpermeability (ARDS) Pulmonary vascular Heart failure with cyanosis Neuromuscular Trauma (head, neck) Ptx, pleurisy Chest wall(deform. , trauma) Drug overdose (sedatives) Type I + + + + Type II + + +
Oxigen supplementation in chronic resp. insuff. NOTT: Ann Intern Med, 1980 BMC: Lancet, 1981 only way to prolong survival in case of chronic resp. insuff. Indication: (stable condition) • Pa. O 2 < 55 mm. Hg or SAT < 88% • 55 mm. Hg < Pa. O 2 < 60 mm. Hg with pulmonary hypertension, polyglobulia or right heart failure Aim: Pa. O 2 ≈ 60 mm. Hg vagy SAT ≈ 90 % CAVE: CO 2 retention in COPD (max. 1 -2 L/min)! Dosage: > 15 h/day
Pa. O 2 < 55 Hgmm Pa. O 2 > 55 Hgmm
ARDS
The causes of ARDS Shock Infection Hematologic Inhalation Ingestion Embolism Metabolic Other Trauma, haemorrhagia, acut hypovolemia (severe burning of the skin) Pulmonary - extrapulm. sepsis DIC, abundant transfusion NO 2, NH 4, Cl, SO 2, gases, O 2 -tox. (FIO 2 >0. 5), gastric acid aspiration Paraquat, barbiturat, aspirin, narcotics, lidocain, hydrochlorotiazid fat, air, cell aggregate Diabetic ketoacidosis, uremia Pancreatitis, height , irradiation, aspiration, drawn in water, re-exspansion
Diagnosis of ARDS • Acute onset (1 -3 days) • One or more risk factors • Chest X-ray: new, bilateral, snow flake – like infiltrates • Exclusion: heart failure, fluid overdose, chronic lung disease • Hypoxemia not corrected with O 2: - mild: Pa. O 2/FIO 2 200 -300 mm. Hg - moderate: 100 -200 mm. Hg - severe: < 100 mm. Hg
Non-invasive ventilation (NIV) in global respiratory insufficiency - Bi. PAP
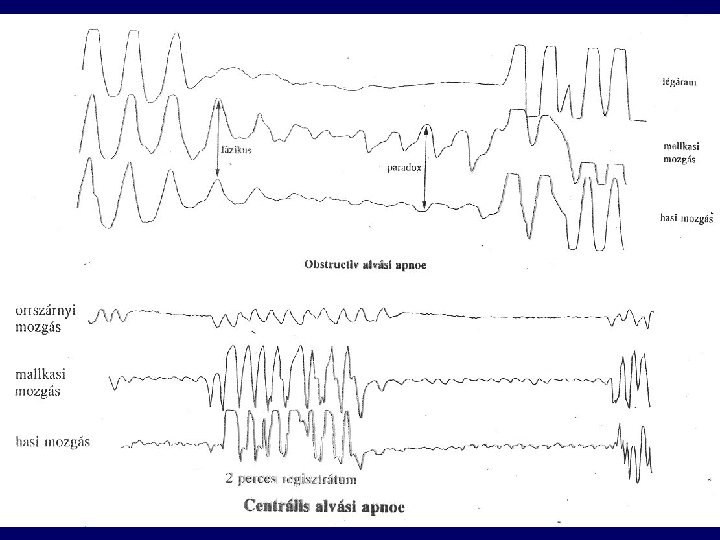
Sleep apnoe-hypopnoe syndrome (SAHS) • Dg: apnoe >5/h , >30/sleep period, SAT decrease: minimum 4% • Apnoe: > 10 s • Arousal (EEG) defraction of sleep • Apnoe index: Number of apnoe/h: <5 - mild: 5 -15 - moderate: 15 -30 - severe: >30
Types of SAHS • Central (kb. 5%) • Obstructive • Mixed Risk factors: - obesity - alcohol - sedatives
Symptoms of SAS • • • Daytime sleepiness Morning headache, tenebrosity Change in personality Strong hoarsness Movements during sleep Enuresis nocturna Impotency Hypertonia, arrhythmias Right heart failure
Score: 0 – 24 Upper limit of normal: 9 Normal : 5. 9 ± 2. 2 SAS: 16 ± 4. 4
Diagnosis of SAS (poliszomnográfia) • • • EEG EOG EMG EKG ABG, pulzoximetry Detection of airflow Detection of breathing movements, leg movements Voice recording Video
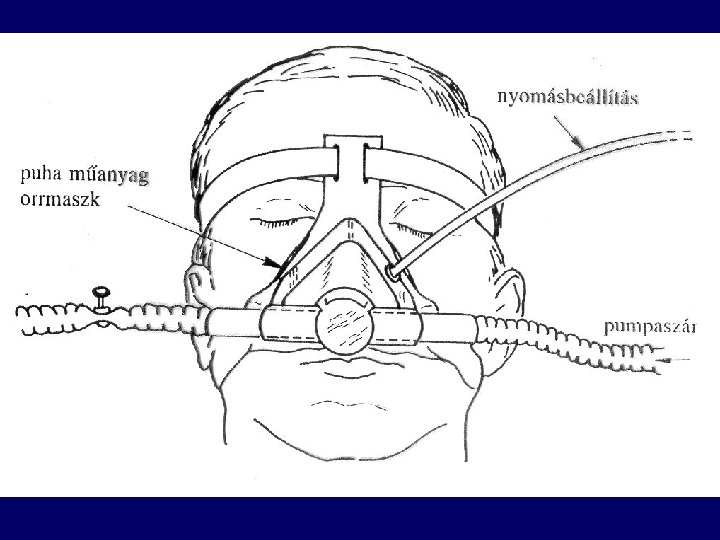
Therapy of SAS • Change in life style • n. CPAP, Bi. PAP • • • Medroxiprogesteron (Provera) Surgery Acetazolamid (Diamox, Fonurit) Almitrin Protryptilin
Effect of c. PAP