Radiological Category Thoracic Chest Principal Modality 1 General
: General Radiography Principal Modality (2): Computed Tomography")



 is a form of pseudotumor that")



- Slides: 11
Radiological Category: Thoracic Chest Principal Modality (1): General Radiography Principal Modality (2): Computed Tomography Case Report #0172 Submitted by: Beth A. Chasen, M. D. Faculty reviewer: Marvin H. Chasen, M. D. Date accepted: 15 February 2005
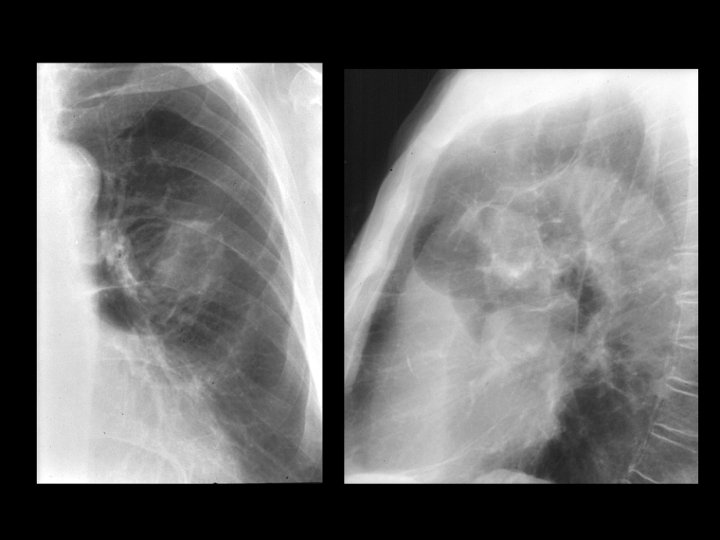
Case History 86 year old male with a lesion discovered on routine chest radiograph. The patient Is asymptomatic and had the study as part of a geriatric workup.
Test Your Diagnosis Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page. • Primary bronchogenic carcinoma • Round pneumonia • Round atelectasis • Metastatic lesion
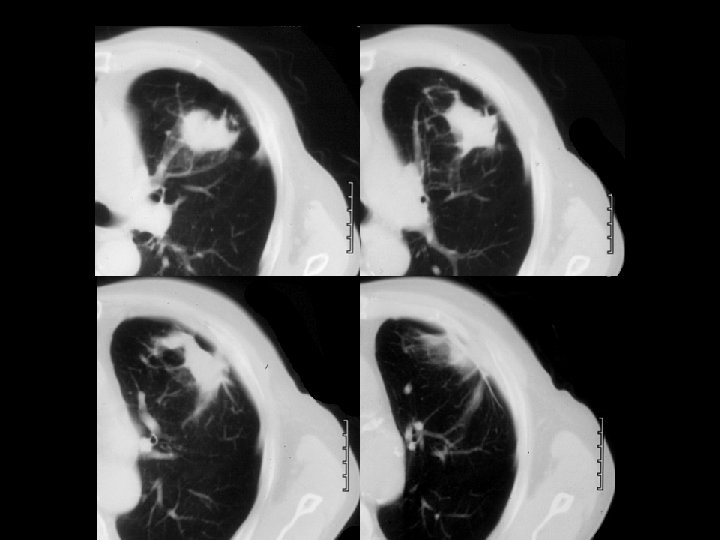
Findings and Differentials Findings: Frontal and lateral chest radiographs demonstrate a 3 -4 centimeter left upper lobe mass with surrounding areas of hyperlucency and arcuate parenchymal distortion. A healed left upper posterior rib fracture is noted. Four CT images show the irregular left upper lobe mass with peripheral attachment to thickened pleura. Note the parenchymal distortion in association with the inferomedial aspect of the lesion. Differentials: • Round atelectasis • Primary bronchogenic carcinoma
Discussion Round atelectasis (also known as rounded atelectasis) is a form of pseudotumor that often mimics a bronchogenic carcinoma. It is most often associated with prior asbestos exposure but can be caused by other insults including trauma. In theory, any process that results in development of a pleural effusion with associated atelectasis can result in round atelectasis. Specifically, if an effusion results in fibrinous adhesions to the atelectatic lung, subsequent lung trapping results in a “rolling up” of this portion of lung. As the effusion clears, the remaining lung in the region re-expands, leaving only the “rolled up”, trapped lung as evidence of prior effusion. Thus, round atelectasis is a peripheral process requiring adhesions with the pleura. As noted in the initial chest radiograph and associated CT images in this case, The arcuate parenchymal distortion in association with the mass represents bronchovascular structures trapped in the “rolled up” atelectatic lung. The inferomedial location of this parenchymal distortion with respect to the hilus of the mass has been termed the comet tail sign. Of the four choices given in the initial diagnosis section, the most likely options are round atelectasis and bronchogenic carcinoma. Round pneumonia is not common in adults, and the mass appearance is overall less typical for metastasis.
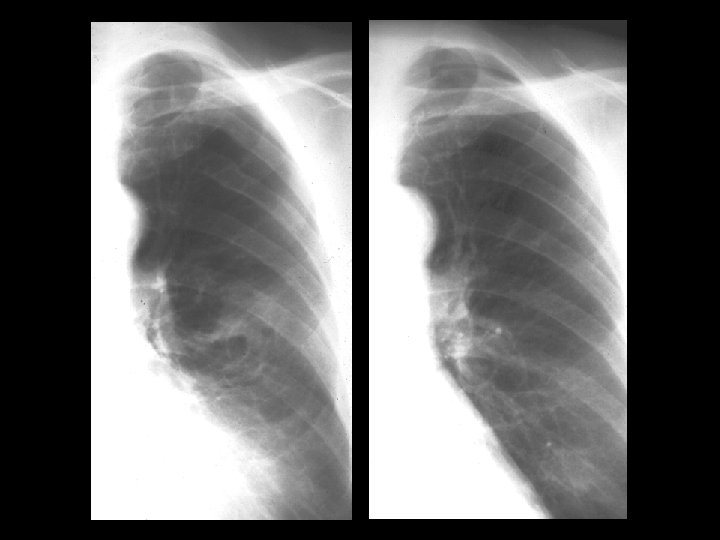
Discussion Further workup of this lesion might include biopsy to determine histology, PET imaging to assess metabolic activity, or observation over time. A valuable clue in this case is the recognition of the healed rib fracture as mentioned in the Findings section of this case. Further investigation of patient history revealed a car accident four years previously. A search for prior studies resulted in review of chest radiographs before and after the accident shown in the subsequent slide:
Discussion Review of the left image obtained two years before the initial images and following the car accident shows healed posterior rib fractures of ribs four and five and an early presentation of the lesion seen lateral to the left hilum. The right image obtained prior to the car accident shows no abnormalities. Therefore, the presumed etiology for development of round atelectasis in this case is prior trauma (rib fracture) with associated hemothorax. References • • • Hanke R, Kretzschmar R. Round Atelectasis. Semin Roentgenol 1980; 15 (2): 174 -182. Schneider HJ, Felson B, Gonzalez LL. Rounded Atelectasis. AJR 1980; 134: 225 -232. Woodring JH. Pleural Effusion is a Cause of Round Atelectasis of the Lung. J Ky Med Assoc 2000; 98 (12): 527 -532.
Diagnosis Round atelectasis resulting from prior trauma