Prognostication and the frail elderly Dr Claire Curtis



































as markers too non-specific Screen for psychological")




- Slides: 41
Prognostication and the frail elderly Dr Claire Curtis Consultant in Palliative Medicine September 2010
Prognostication and the frail elderly n n Introduction Prognostication Advance care planning Symptom control
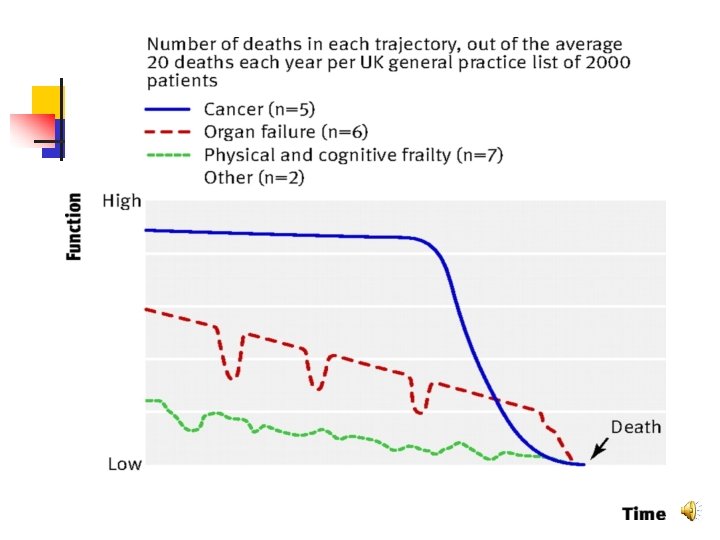
Introduction n n Aging population Proportion of people over 60 will rise from 10% to 22% in 2050 UK – 83% of deaths are in people >65 Difficult to identify when “End of Life” starts Prolonged uncertain trajectory of dying
Prognostication - importance n Doctors n n Patients n n n Inform clinical decisions Inform care decisions - CHCF Inform patient and relatives (difficult questions) Inform decisions/goal setting/expectations Future planning – finances/family/place of care Relatives n n Inform decisions - work/finances Preparedness/saying goodbye
Prognostication – are we any good? n n Physicians dislike doing it, tend to be optimistic and overestimate Predication of survival improves over time n n Increasing knowledge of the patient Worsening illness Increasing experience of doctor Accurate in predicting imminent death
Prognostication n n Subjective decision from experienced clinician about prognosis is as accurate as tools focusing on performance status, symptoms and simple lab tests (albumin) Can be helpful to have some guides
Prognostication n Difficult n n n Cancer Progressive disease Frailty
Prognosis - cancer n n Clearer trajectory 5 year survival rates, median survival known Variety of prognostic research tools Performance status, biological markers (CRP, albumen)
Prognosis – non-cancer n n Disease specific tools PIG n n n Heart failure COPD Renal failure Parkinson’s Mnd/ms
Frailty n n n Progressive physiological process marked by declines in function and reserves as well as increased vulnerability to morbidity and mortality Often seen but not recognised (leads to unnecessary investigations) Clinically n n n Generalised weakness Weight loss Fatigue Slowed performance Generalised state of low activity
Frailty Gradual progressive downward spiral n Inability to recover from trivial illness n Confusing for families n Increased risk of death (when all other factors controlled) similar to metastatic cancer or heart failure n
GSF Prognostic indicator: Frailty n n Multiple co morbidities with signs of impairments in day to day functioning At least 3 of: n n n Weakness Slow walking speed Low physical activity Weight loss (>10% over 6 months, also albumin <25 g/l)) Self reported exhaustion Deteriorating Karnofsky score (= deteriorating performance status)
Karnofsky score n Measures patient performance of activities of daily living: n 100 80 n 60 n n 40 20 n 10 n Normal activity with effort, some symptoms Require occ assistance, cares for most needs disabled, requires special assistance Very sick, requires active supportive treatment Moribund
Barthel Index n Assesses individual’s ability to perform activities of daily living n n n n Personal care Mobility and transfers Bathing and feeding Each task scored individually and totalled 100 = maximum independence 0 = total dependence A low initial score and a decline of 10 points or more in a week indicative of short prognosis (2 -3 weeks)
When to think about prognosis n n n n Surprise question Prognostic markers – for specific diseases New diagnosis of life limiting condition Step change in treatment Multiple hospital admissions Admission to care home Whenever a thorough reassessment of need is required, inc death of a spouse
Advance care planning n n n “Hoping for the best, preparing for the worst” – not to take away hope Process of discussion between an individual and their care providers to make clear a person’s wishes Most effective when physician and patient work together Clinicians tend to underestimate patient's desire for info, overestimate what the patient has understood and their desire to make decisions A process, with time between discussions Patient should feel in control of timing, place and pace of discussion with option to stop at any time
Barriers to EOL communication n n Difficult subject Variation in patient preferences for info and discussion Perception that dr does not want/has no time for discussion Fear of removing hope, causing alarm or distress Emphasis on curative model of care Unfamiliar faces Multiple healthcare teams Unpredictability of illness Inadequate communication skills of professionals Delirium/confusion/fatigue/breathlessness/depression
Facilitators to EOL communication n n n Patient experience of family/friends who have died Trusting ongoing relationship with dr Patient feeling cared for as a person Doctor asks about EOL care skilfully Patient had discussed EOL care with others previously Patient experience of being very ill Health systems that expect drs to have EOL discussions with patients
How to communicate prognosis n n n Be honest and direct Make it clear Show you care Give time Pacing information Staying the course (doctor won’t abandon patient as illness progresses)
Documentation of discussions n Advance statement Advance decision to refuse treatment Lasting power of attorney DNAR n Sharing of information n n Treatment and care towards the end of life: good practice in decision making. GMC Publications May 2010
Advance statement n n n Covers an individual’s preferences, wishes, beliefs, values To guide future best interests decisions in the event an individual has lost capacity Makes MDT aware of the patient’s wishes Might mention who to consult if a decision has to be made (but they cannot make the decision) Not legally binding but must be taken into account when acting in a patient’s best interests
Advance decision to refuse treatment n n n Can only cover refusal of a specified future treatment in the event that an individual has lost capacity to make that decision Cannot refuse basic nursing care and comfort measures Cannot demand care Cannot be made if lack of capacity For refusal of life sustaining treatment, must be written, signed and witnessed and contain a statement that it applies even if the person’s life is at risk Legally binding
Symptom control in frail elderly n n Principles the same as for younger patients But: n n n How much to investigate? Multiple co-morbidities Polypharmacy Renal and liver function Increased variability of repsonse to drugs
Prevalence of complaints >75 yrs n Health complaint clusters: n n n n Communication problems – 80% Mobility problems – 70% Digestion problems – 65% Psychosocial problems – 60% Elimination problems – 55% Circulatory problems – 50% Focus on symptom management rather than on the diseases
Geriatric syndromes in palliative medicine n n n Frailty Dementia Delirium Constipation Falls Depression
Aims - frailty n Control pain and other symptoms n n Uncontrolled pain ass with increased frailty Preventing hospital admission Maintaining and improving functional status (rehab and exercise) Improving overall sense of wellbeing – psychological and social interventions
Dementia Not a dementia talk n Symptoms vary between forms of dementia n Behavioural changes n n Paranoia, delusions, hallucinations, sleep disorders, agitation Cognitive and functional decline Needs vary as disease progresses
GSF Prognostic indicator: Dementia n n n n Unable to walk without assistance Urinary and faecal incontinence No consistently meaningful verbal communication Unable to dress without assistance Barthel score <3 Reduced ability to perform activities of daily living Plus any 1 of: n 10% wt loss in prev 6 mths, pyelonephritis or UTI, albumin 25 g/l, severe pressure sores, recurrent fevers, reduced oral intake, aspiration pneumonia
Delirium n n n Confusion Acute onset and fluctuating course And Inattention – And either Disorganised thinking - or Altered level of consciousness
Delirium n n n High prevalence Associated with increased morbidity, mortality and hospital admission 2 forms n n n Many causes n n Infection, metabolic, drugs, hypoxia, constipation, urine retention, pain Prevention n Hyperactive, hyperalert Hypoactive, hypoalert Education Good nursing care inc hydration, bowels Recognition n Can be reversible, may not be “actively dying”
Delirium: treatment n n Treat the underlying cause Who to sedate? n n n Those with distressing hallucination/delusions Distressing agitation Behaviour which puts others at risk n n n There is no drug which will make a wandering patient sit quietly by their bed Low dose Haloperidol – 500 mcg – 1 mg bd orally Not for patients with Parkinsons, use low dose Lorazepam instead
Constipation n n Very common Lots of causes n n Complications n n n Medication, chronic disease (DM, hypothyroid, IBS) Functional bowel obstruction Nausea/vomiting/anorexia Delirium Colonic perforation Guidelines
Constipation - treatment n Softner n Sodium docusate 100 -200 mg bd or Movicol 1 -2 sachets/day PLUS n Stimulant n Bisocodyl 5 -10 mg od or Senna 7. 5 -15 mg od OR n Combined softner and stimulant n n Co-danthramer 1 -2 capsules at night (do not use if colostomy or at risk of incontinence) Titrate oral laxatives to maximum
Constipation - treatment n n Digital rectal exam if BNO (72 hrs at minimum dose) Hard Faeces n n Soft Faeces n n Glycerin suppository +/- bisacodyl suppository Bisacodyl suppository or sodium citrate enema (Microlax) No Faeces n Phosphate enema (patient to lie on left side, to be given before 18: 00
Falls n Vicious cycle n n n Fall – fear of fall – change of gait – reduced mobility – increased falls May be a sign of worsening disease (prognostication) Multifactoral n Medication, medical disease, environment, sensory impairment, decreased strength, impaired gait
Depression n n Frequent Symptoms (anorexia, insomnia etc)as markers too non-specific Screen for psychological symptoms eg hopelessness, guilt, suicidal ideation Screening questions n n Are you depressed? During the past month have you often been bothered by feeling down, depressed or hopeless? During the past month have you often been bothered by little interest or pleasure in doing things?
Oral intake n Dysphagia n Part of disease process n n n Poor dentition Xerostomia n n n Cancer, neurological condition Multifactorial – often medication, blunted thirst response in elderly, age related conditions eg DM, infection, Sjogren’s Environmental – lack of assistance, poor diet Loss of appetite normal part of all terminal conditions including frailty Don’t suffer hunger Dry mouth helped by oral hygiene, artificial saliva, sips of water No evidence that artificial hydration or nutrition prolongs life or relieves suffering in patients with terminal dementia or other illnesses
Conclusion n n Aging population Prognostication important n n Advance care planning n n Difficult in non-malignant disease Communication Symptom control n Frailty, Dementia, Delirium, Constipation, Falls, Depression
“I think the best physician is the one who has the providence to tell the patient according to his knowledge of the present situation, what has happened before, and what is going to happen in the future” Hippocrates (470 -410 BC)
References n n n Prognostic indicator paper vs. 2. 25, GSF Programme, England, June 2006 Editorial. Payne s, Frogatt K. International Journal of Palliative Nursing, 2006, Vol 12, No 5 Advance care planning. Kite S. Clinical Medicine 2010, Vol 10, No 3: 275 -8 Accuracy of prediction of survival by different professional groups in a hospice. D. Oxenham, Palliative Medicine 1998 An audit of the use of the Barthel Index in palliative care. International journal of palliative nursing 2007: Vol 13, No 11 543 -48 Palliative care as a framework for older people’s long term care. Hallberg. International journal of palliative nursing 2007: Vol 13 No 11: 224 -229