Colorectal Cancer in Older Patients Key Issues Etienne

 •")

 • Treatment according guidelines =")










")

 –")

- Slides: 20
Colorectal Cancer in Older Patients Key Issues Etienne GC Brain, MD Ph. D Institut Curie Saint-Cloud, France www. siog. org etienne. brain@curie. fr 1
Epidemiology • 23 -45% digestive tumours are diagnosed > 75 yo (FRANCIM 2010) • CRC (INCa 2012) – – – 75 -84 yo 14. 7% of all cancers > 85 yo 18. 7% of all cancers 1 st cancer any sex in elderly 30% new cases 75 -84 yo Median age at diagnosis 70 yo Screening > 75? ? ?
• 28 independent studies & 34 194 patients • Older patients – – – Increased frequency of comorbid conditions More later-stage disease More emergency surgery Less curative surgery More postoperative morbidity and mortality Worse OS but less striking for CRC-specific survival Lancet 2000
Undertreatment • 110 cases > 75 yo (1995 -2000) • Treatment according guidelines = 48% pts – Surgery – Chemotherapy • III • IV 87% (R 0 56%) 26% 17% – XRT (rectum) • Early stage • Palliative 17% 21% Apparicio CROH 2009
Doat Eur J Cancer 2014
75+ vs < 75: median OS 8. 4 months vs 22. 3 months (17. 1 months in 75+ w/ chemo) Doat Eur J Cancer 2014
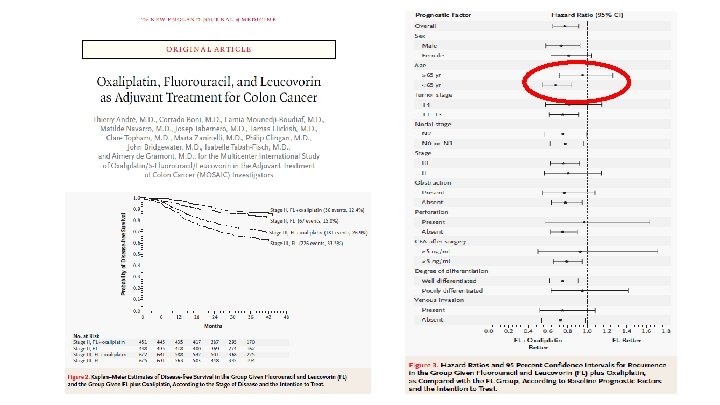
Adjuvant Setting Sargent NEJM 2001
• • Benefits of oxaliplatin beyond fluoropyrimidine in pts > 70 years is uncertain Increased risk for AE’s with combination chemo (25% SAE w/ 15% neuropathy) – Decision based on clinician’s clinical judgment – Recurrence risk • Fluoropyrimidine monotherapy is appropriate when oxaliplatin is felt to add excessive risk of toxicity for a patient 20
Questions • Stratification on frailty/life expectancy for oxaliplatin vs none or chemo ves none (ADAGE/PRODIGE 34) • Deficiency in mismatch repair & MSI (high frequency in older patients and improved prognosis)? 21
Metastatic Setting • Most studies show similar benefit to systemic treatments as younger patients • Few specific studies in older patients – FOCUS 2, FFCD, AVEX • Chemo – Mono vs bi-therapy (oxaliplatin, irinotecan) – ! Capecitabine > 70 • Targeted treatments – Anti-EGFR, anti-VEGF – ! Bevacizumab with ATE history
Frail and elderly • • R 1: 1: 1: 1 Stratification: centre, PS, surgery of primary, age B : FOLFOX q 2 w C : capecitabine q 3 w to le ra nc e go Do In se > itia 6 l: w: 80 10 % 0% if A : LV 5 FU 2 q 2 w od PS: FOCUS 1 (Fluorouracil, Oxaliplatin, CPT 11 [irinotecan]: Use and Sequencing): median age 64 yo (vs 60% deaths > 75+) (Lancet 2007) D : XELOX q 3 w Primary objective: Overall Treatment Utility = oxaliplatin and PFS (A vs B + C vs D), capecitabine and Qo. L (A vs C et B vs D) Secondary objectives: RR, toxicity, OS Statistics: 2 x 2, PFS 6 vs 9 mth, α 5% β 20%, Qo. L 40% vs 60% improvement at 12 w, α 5% β 10%, 460 patients
• Oxaliplatine – – • 5 FU – • QOL mprovement by 56% w/FU or capecitabine More AE grade ≥ 3 if – – • Median PFS 5. 8 [3. 3 -7. 5] vs 4. 5 [2. 86. 4], HR 0. 84 (0. 69 -1. 01, p = 0. 07) More RR 41 -54% vs 35 -37%) Oxaliplatin Cape 39% vs 32% p = 0. 17 40% vs 30% p = 0. 03 Multivariate – Less symptoms – Limited disease – Oxaliplatine Better OTU
FFCD 2001 -02 • 123 patients with m. CRC, first line of chemotherapy – – – • 75% 31% 34% Toxicity – – – • 5 -FU-based chemo ± irinotecan Median age 80 yo (75 -91) Charlson index≤ 1 MMSE ≤ 27/30 IADL impairment grade 3 -4 toxicity • 71 patients (58%): IRI, MMSE, IADL Dose-intensity reduction > 33% • 41 patients (33%): IRI, Alk phosph ≥ 1 unexpected hospitalization (4 mth) • 54 patients (44%): MMSE, GDS Cognitive function and autonomy impairment should be taken into account when choosing a regimen for chemotherapy Aparicio J Clin Oncol 2013
Cunningham Lancet Oncol 2013
AVEX • PFS: 9. 1 vs 5. 1 mos (HR 0. 53, p<0. 001) • OS: 20. 7 vs 16. 8 mos (HR 0. 79, p=0. 182) – [AVF 2107 g results: IFL+/- BEV 20. 3 mos vs 15. 6 mos (HR 0. 66, p<0. 001)] • RR: 19. 3% vs 10% p=0. 042 • Grade 3+ AEs: 59% vs 44. 1% • Conclusions: Cape + BEV could be a standard for selected elderly patients Cunningham Lancet Oncol 2013
• SEER database • 3, 039 patients ≥ 66, stage IV breast, lung, colon cancer, 2004 -2007, bevacizumab – Contra-indication defined as 2 claims for thrombosis, cardiac disease, stroke, hemorrhage, hemoptysis, or GI perforation – Toxicity defined as 1 st development of 1 condition > beva – Beva use associated w/ white race, later year of diagnosis, tumor type, and decreased comorbid conditions – 35. 5% had contra-indication • Black race, increased age, comorbidity, later year of diagnosis, lower socioeconomic status, lung and CRC – If no contra-indication 30% complication (black race) 42 Hershman J Clin Oncol 2013
Cetuximab • Pooled analysis from KRAS wild-type pts – CRYSTAL (FOLFIRI +/- cetuximab) – OPUS (FOLFOX +/- cetuximab) • OS, PFS and safety were all similar among older ( ≥ 70 years) and younger (<70 years) pts. • Grade 3+ toxicity was increased in both treatment arms for elderly patients – NO obvious interaction between age (< 70 vs ≥ 70 years) and the differences for treatment toxicity between the arms. Folprecht ESMO 2010
• • Treatment decisions should not be based on age alone Fit older patients can tolerate combination cytotoxic therapy as well and benefit as much as younger patients – Same for biologics • Consider less intense regimens for those who are not candidates for standard regimens – Reduced dose FP + oxaliplatin – Cape + BEV