Methicillinresistant Staphylococcus Aureus MRSA not just a healthcare
: not just a healthcare associated multi-drug resistant pathogen anymore")




 S. aureus(MRSA • Has a mec. A gene which is")

 • A mobile genomic island where mec. A gene")





risk of developing a subsequent")






- Slides: 21
Methicillin-resistant Staphylococcus Aureus - (MRSA): not just a healthcare associated multi-drug resistant pathogen anymore Presenter: Zipporah Machuki
Background S. aureus : • Facultative anaerobic • gram-positive coccal bacterium. • forms large, round, golden-yellow colonies on BA often with hemolysis. • Reproduces asexually by binary fission • cells are arranged in cluster. • catalase-positive, • coagulase test was used to differentiate S. aureus from other staphylococci epidermidis. However it is now known that not all S. aureus are coagulase-positive.
• S. aureus commonly colonizes • Survives for a long time on skin or environment. • Mortality 80% prior to introduction of Penicillin. • Resistance to penicillin usually mediated by beta-lactamase,
Methicillin • A penicillinase-resistant penicillin • First used in 1959 and • 2 years later S. aureus developed methicillin-resistance. • Due to acquisition of the mec. A gene. • Traditionally recognized as a nosocomial pathogen • Epidemiology has radically changed
Mode of action of methicillin • Bind to the native PBPs that are present in the S. aureus cell wall • Leads to the disruption of the synthesis of the peptidoglycan layer and therefore lysis of the S. aureus.
Methicillin Resistant S. aureus(MRSA) S. aureus(MRSA • Has a mec. A gene which is 2. 1 kb in length • mec. A gene codes for the 78 -k. Da penicillin binding protein (PBP) 2 a (or PBP 2’), • PBP 2 has decreased affinity for most beta -lactam antibiotics.
Mechanism of resistance • When PBP 2 a is produced, • the binding of the b-lactam antibiotics is hindered and • PBP 2 A (a transpeptidase), assisted by the transglycosylase domain of the native PBP 2 of S aureus, takes over the function of biosynthesis of cell-walls • Result in the growth of MRSA
staphylococcal cassette chromosome mec (SCCmec) • A mobile genomic island where mec. A gene is located. • Carries chromosome recombinances genes called ccr. A/ccr. B and ccr. C that enable excision and intergration into the host chromosome. • seven types main of SCCmec (SCCmec I to VII)
Epidemiology of MRSA • MRSA first identified in 1960 • became a common nosocomial infection in 1980. • Previously known to be only a nosocomial pathogen. • Risk factors associated with development of MRSA infections: (i) surgery, dialysis, hospitalization or residence in a long-term care facility within the prior year; (ii) indwelling percutaneous devices such as central venous catheters or feeding tubes; (iii)an MRSA infection identified more than 48 hours after hospital admission; or (iv)Had previously had. MRSA cultured
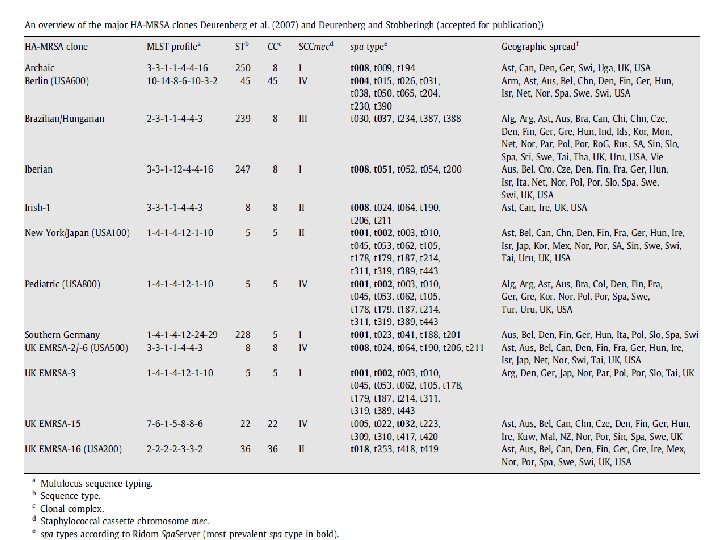
• MRSA cultured from patients with these risk factors are known as HA-MRSA. • major clones that disseminated internationally: Iberian, v Brazilian, v Hungarian, v New York/Japan, and v Paediatric clones • CA-MRSA is cultured from healthy and young individuals without any of these clinical risk factors.
Control of HA-MRSA • Screening of staff Health-care workers who are nasal carriers can serve as sources of MRSA transmission, • Isolation and barrier nursing Patients colonised or infected with MRSA • Hand hygiene Transient contamination of health-care workers’ hands • Environmental cleaning How important are contaminated environmental surfacesas a reservoir for MRSA?
Treatment of HA-MRSA • • Laptomycin, Linezolid, Tigecycline and Vancomycin Zhanel et al. 2013
Differences between HA-MRSA and CA-MRSA Bassetti M et al 2009
Transmission of CA-MRSA • colonize the nose and nares (Reservoir)risk of developing a subsequent infection is 10. 7% (Ellis MW 2 et al 200) • Transmission between individuals is likely to be facilitated by: v crowded living conditions, vactivities that involve skin-to-skin contact, v poor hygiene practices and vsharing of contaminated household items (towels, combs etc. ).
Groups at risk of CA-MRSA Zetola N et al 2005
CA-MRSA causes: • skin and soft tissue infections and • invasive disease such as vsepsis and vnecrotizing pneumonia
o Skin and Soft Tissue Infection Most common manifestation of CA-MRSA, -particularly abscess or furunculosis o Necrotising pneumonia Caused by PVL gene-positive CA-MRSA strains o Osteoarticular Infections Common in children o Other Infections Infective endocarditis Sepsis is a complication of CAMRSA disease
Treatment of CA-MRSA Infections • There is no defined optimum management of CA-MRSA infections. • Current strategies include a combination of pharmacological and nonpharmacological intervention eg In patients with recurrent infections, attempts to decolonize CA-MRSA
Commonly used antibiotic Agent comment Ceflobiprole Not yet widely availabel Clindamycin i. MLSβ resistance my reduce activity Daptomycin 6 mg/kg IV indicated for bacteraemia; do not use to treat pneumonia Linezolid Not recommended to treat bacteraemia Quinupristin/dalfopristin i. MLSβ resistance my reduce activity Tigecycline Tlow serum concentration so not recommended for bacteraemia treatment Cotrimoxazole Activity against GAS is unknown; Not for use in infants aged <2 mo or during 3 rd trimester of pregnance. Vanomycin Requires monitoring concentration when treating serious infections