Empiric Treatment Pneumonia Overview of Pneumonia http www










: individual residing in their homes •")



 • Aminopenicillins: Ampicillin (high")








 Macrolide + -lactam Doxycycline")





 • Ampicillin/sulbactam")









")



 • Quinolones: Ciprofloxacin,")



 Vaginal")













,")











 – Antistaphylococcal penicillins (Dicloxacillin) – First")
 – Antistaphylococcal penicillins (Nafcillin, oxacillin) –")


 • Hearing Loss • Irritability •")



")

























 • Carbapenems (imipenem, meropenem)")

- Slides: 118
Empiric Treatment: Pneumonia
Overview of Pneumonia • http: //www. virtualrespiratorycentre. com/ diseases. asp? did=38 • Link • LINK
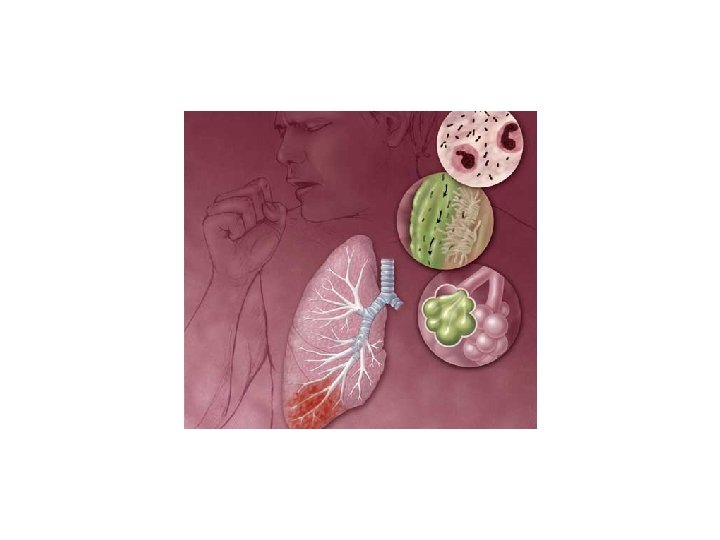
What is pneumonia? • Pneumonia is an inflammatory illness of the lung.
Frequently, pneumonia is described as lung parenchyma/alveolar (microscopic air-filled sacs of the lung responsible for absorbing oxygen from the atmosphere) inflammation and (abnormal) alveolar filling with fluid.
What Causes Pneumonia? • Pneumonia can result from a variety of causes, including infection with bacteria, viruses, fungi, or parasites, and chemical or physical injury to the lungs.
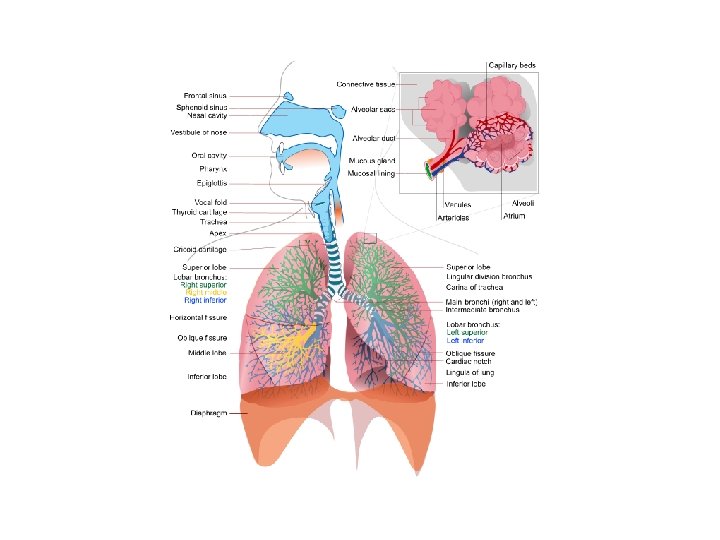
Pneumonia • The alveoli are tiny air sacs within the lungs where the exchange of oxygen and carbon dioxide takes place.
• Bronchiole: A tiny tube in the air conduit system within the lungs that is a continuation of the bronchi and connects to the alveoli (the air sacs where oxygen exchange occurs. • Bronchiole is the diminutive of bronchus, from the word bronchos by which the Greeks referred to the conduits to the lungs.
Symptoms of Pneumonia • • Fever Chills Cough Pleurisy: inflamed membranes around the lungs • Dyspnea: Difficult or labored breathing; shortness of breath
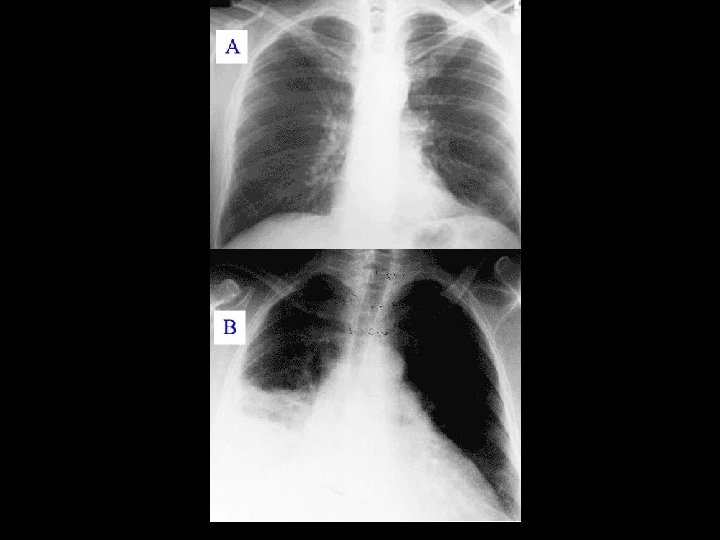
Diagnosis of Pneumonia • Pneumonia usually produces distinctive sounds; these abnormal sounds are caused by narrowing of airways or filling of the normally air-filled parts of the lung with inflammatory cells and fluid, a process called consolidation.
Diagnosis of Pneumonia • In most cases, the diagnosis of pneumonia is confirmed with a chest x-ray. • For most bacterial pneumonias, the involved tissue of the lung appears on the x-ray as a dense white patch (because the x-ray beam does not get through), compared with nearby healthy lung tissue that appears black (because the x-rays get through easily, exposing the film). • Viral pneumonias typically produce faint, widely scattered white streaks or patches.
Two Types of Pneumonia • Community-Acquired Pneumonia (CAP): individual residing in their homes • Hospital-Acquired Pneumonia (HAP): individuals residing in hospitals
Community-Acquired Pneumonia • Typical: Sudden onset of fever, chills, pleuritic chest pain, productive cough – Streptococcus pneumoniae – Haemophilus influenzae • Atypical: often preceded by mild respiratory illness – Legionella spp. – Mycoplasma pneumoniae – Chlamydophila pneumoniae
CAP: typical Streptococcus pneumoniae Gram + Usually susceptible to penicillin
Streptococcus pneumoniae
Treatment of Streptococcus pneumoniae Ampicillin • Penicillin G (high doses) • Aminopenicillins: Ampicillin (high doses)
Treatment of Penicillin-resistant Streptococcus pneumoniae • Second Generation Cephalosoporins: Cefuroxime • Third Generation Cephalosporins: Cefotaxime, Ceftriaxone • Quinolones: Moxifloxacin, Levofloxacin • Vancomycin • Macrolides/ketolines: Telithromycin
Haemophilus influenzae
Haemophilus influenzae • Haemophilic means ‘blood loving’. The organism requires a blood-containing medium for growth • Influenzae: The bacterium often attacks the lungs of a patient with viral influenza. • Since the organism was frequently isolated from the lungs of patients during the 1890 and 1918 influenza pandemics, scientists incorrectly concluded that the bacterium was the causative agent.
Haemophilus influenzae
Haemophilus influenzae
Treatment of Infections Caused by Haemophilus influenzae • Aminopenicillins + -lactamase inhibitor: – Amoxicillin/clavulanate – Ampicillin/sulbactam • Second-generation cephalosporin – Cefuroxime • Third-generation cephalosporin – Ceftriaxone – Cefotaxime
Bacterial Causes of CAP • • Streptococcus pneumoniae Haemophilus influenzae Legionella spp Mycoplasma pneumoniae Other aerobic Gram-neg Chlamydophila pneumoniae Staphylococcus aureus 16 -60% 3 -38% 2 -30% 1 -20% 7 -18% 6 -12% 2 -5%
Treatment of CAP
Treatment of CAP • Mild – – Macrolide (azithromycin, clarithromycin) Macrolide + -lactam Doxycycline Quinolone (moxifloxacin, levofloxacin, gemifloxacin) • Severe – -lactam + macrolide – -lactam + quinolone
Treatment of CAP • Severe – -lactam + macrolide – -lactam + quinolone
HAP is also divided into two classes: • Early onset HAP: occurs within first five days of hospitalization • Late onset HAP: occurs after 5 days of hospitalization
Bacterial Causes of Early Onset HAP • • Methicillin-sensitive Staphylococcus aureus Haemophilus influenzae Enterobacteriaceae Streptococcus pneumoniae 29 -35% 23 -33% 5 -25% 7 -23%
Bacterial Causes of Late Onset HAP • • Pseudomonas aeruginosa Acinetobacter spp. Enterobacteriaceae Methicillin-resistant S. aureus 39 -64% 6 -26% 16 -31% 0 -2%
Treatment of Early Onset HAP Ceftriaxone = 3 rd gen. cephalosporin
Treatment of Early Onset HAP • Ceftriaxone • Quinolone (Levofloxacin, Moxiflocacin, Ciprofloxacin) • Ampicillin/sulbactam • Ertapenem
Treatment of Late Onset HAP
Treatment of Late Onset HAP Use a combination regimen from the first and second categories below: • Antipseudomonal cephalosporin: ceftazidime, cefepime • Or Carbapenem: Imipenem, Meropenem • Or Extended spectrum penicillin/ -lactamase inhibitor: piperacillin/tazobactam ++++ • Quinolone (ciprofloxacin, levofloxacin) • Or Aminoglycoside (gentamicin, tobramycin, amikacin) • If MRSA is suspected, add: Vancomycin or Linezolid
Urinary Tract Infections • http: //www. virtualrenalcentre. com/disea ses. asp? did=281
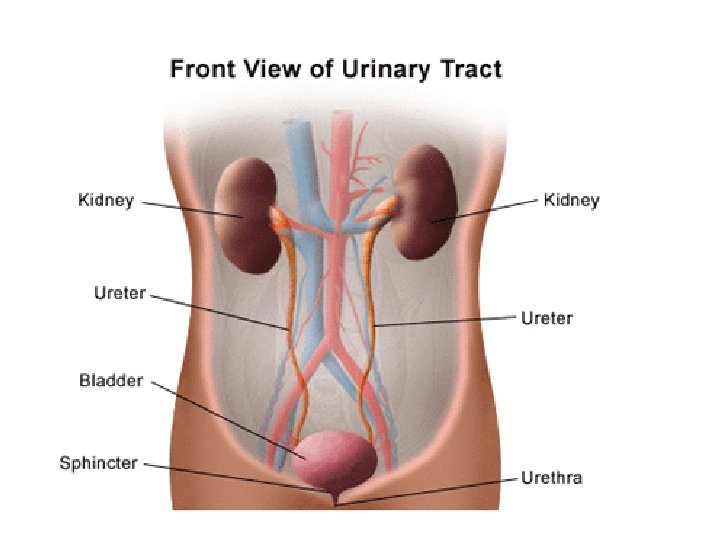
Urinary System
Mild and Severe UTI’s • Mild – Involve only the urethra and bladder – Referred to as “acute cystitis” – Symptoms include • dysuria (painful urination) • urinary frequency • hematuria (blood in urine)
Severe UTI’s • Severe – Infection of the upper urinary tract involves the spread of bacteria to the kidney – Symptoms include fever, chills, nausea, vomiting and flank pain – Called “pyelonephritis”
‘Complicated’ and ‘Uncomplicated’ UTI’s • Uncomplicated: Less likely to recur. Occur in young, healthy, nonpregnant women • Complicated: All other UTI’s. More likely to recur.
Bacterial Causes of Uncomplicated UTI’s • • • Escherichia coli Proteus mirabilis Staphylococcus saprophyticus Klebsiella spp. Other Enterobacteriaceae 53 -79% 4 -5% 3% 2 -3% 3%
Treatment of Uncomplicated Acute Cystitis
Treatment of Uncomplicated Acute Cystitis • Oral trimethoprim-sulfamethoxazole • Oral quinolones (ciprofloxacin, levofloxacin)
Treatment of Uncomplicated Acute Pyelonephritis Amoxicillin, an aminopenicillin Gentamycin, an aminoglycoside
Treatment of Uncomplicated Acute Pyelonephritis • Quinolones: Ciprofloxacin, levofloxacin • Third generation cephalosporins: Ceftriaxone, cefotaxime, ceftizoxime • If Gram positive organisms seen in urine: – Aminopenicillin (amoxicillin) – Aminopenicillin + -lactamase inhibitor: (amoxicillin + clavulanate) – Aminopenicillin + aminoglycoside (ampicillin + gentamicin)
Treatment of Complicated Urinary Tract Infections
Treatment of Complicated Urinary Tract Infections • Fourth generation cephalosporins (cefepime) • Quinolones: Ciprofloxacin, Levofloxacin • If Gram-positive bacteria seen in urine: – Aminopenicillin + aminoglycoside: Ampicillin + gentamicin
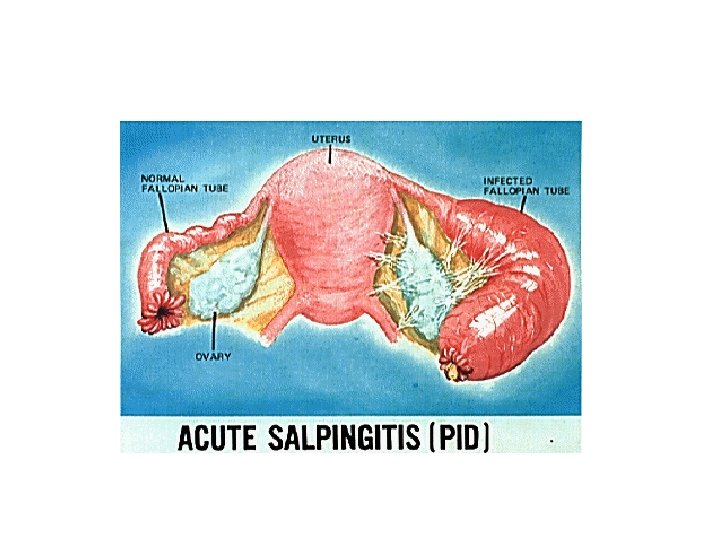
Pelvic Inflammatory Disease • Link
Female Reproductive Organs
PID is the general term for an infection that has traveled through the vagina, to the uterus, and then to other parts of the pelvis
Symptoms of PID • • • Abnormal bleeding Dyspareunia (pain during sexual intercourse) Vaginal discharge Lower abdominal pain Fever chills
Bacterial Causes of PID • Neisseria gonorrhoeae 27 -56% • Chlamydia trachomatis 22 -31% • Anaerobic and facultative bacteria (Bacteria that can live under aerobic or anaerobic conditions) 20 -78%
Treatment of PID
Treatment of PID • Mild to Moderate Disease – Oral quinolone: Levofloxacin, ofloxacin + oral metronidazole – Single IM dose of cephalosporin + oral doxycycline + oral metronidazole
Treatment of PID Those that are severely ill should be admitted to the hospital and treated initially with intravenous agents. • Severe Disease (regimen 1) – Cephalosporin with anaerobic activity (cefotetan, cefoxitin) + doxycycline (active against atypical C. trachomatis) • Severe Disease (regimen 2) – Clindamycin (active against C. trachomatis and against many anaerobes) + Gentamicin (effective against Gram-negative N. gonorrhoeae)
Meningitis • Link
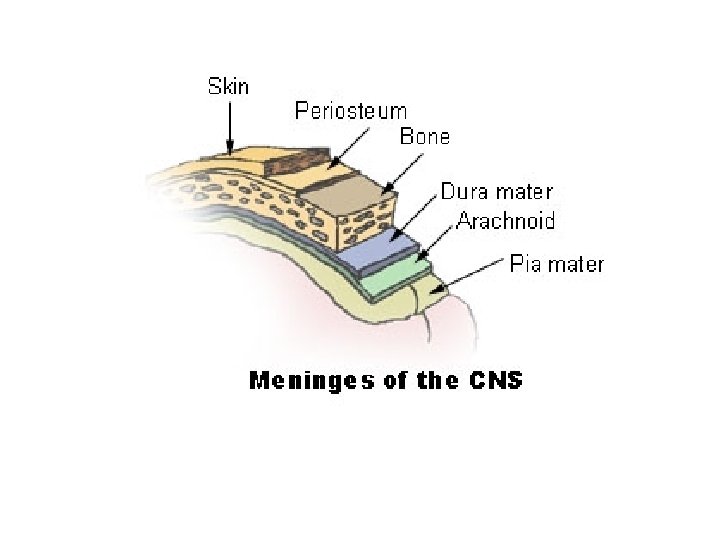
Meningitis • Meningitis is the inflammation of the protective membranes covering the central nervous system, known collectively as the meninges.
• Meningitis may develop in response to a number of causes, most prominently bacteria, viruses and other infectious agents, but also physical injury, cancer, or certain drugs.
• Meninges: the membranes that envelope the brain and the spinal cord.
Symptoms of Meningitis • • Headache Fever Neck stiffness Altered mental status Photophobia Nausea Vomiting Seizures
• The most important test used to diagnose meningitis is the lumbar puncture (commonly called a spinal tap). • Lumbar puncture (LP) involves the insertion of a thin needle into a space between the vertebrae in the lower back and the withdrawal of a small amount of CSF.
Lumbar puncture • http: //www. virtualcancercentre. com/inve stigations. asp? sid=13
Diagnosis of Meningitis • The CSF is then examined under a microscope to look for bacteria or fungi. • Normal CSF contains set percentages of glucose and protein.
• These percentages will vary with bacterial, viral, or other causes of meningitis. • For example, bacterial meningitis causes a greatly lower than normal percentage of glucose to be present in CSF, as the bacteria are essentially "eating" the host's glucose, and using it for their own nutrition and energy production.
Diagnosis of Meningitis • Normal CSF should contain no infection-fighting cells (white blood cells), so the presence of white blood cells in CSF is another indication of meningitis.
• Some of the withdrawn CSF is also put into special lab dishes to allow growth of the infecting organism, which can then be identified more easily. • Special immunologic and serologic tests may also be used to help identify the infectious agent. • LINK
Bacterial Causes of Acute Bacterial Meningitis • 0 - 3 months: – Streptococcus agalactiae – Escherichia coli – Listeria monocytogenes
Bacterial Causes of Acute Bacterial Meningitis • 3 month - 6 yrs: – Neisseria meningitidis – Streptococcus pneumoniae – Haemophilus influenzae
Bacterial Causes of Acute Bacterial Meningitis • 16 yrs - 50 yrs – Streptococcus pneumoniae – Neisseria meningitidis
Bacterial Causes of Acute Bacterial Meningitis • > 50 yrs – Streptococcus pneumoniae – Listeria monocytogenes – Aerobic Gram-negative bacilli
Treatment of Bacterial Meningitis
Treatment of Bacterial Meningitis • Third-generation cephalosporins: cefotaxime, ceftriaxone + Vancomycin (coverage against resistant Streptococcus pneumoniae) • If patient < 3 months or > 50 years Same as above, but also Add ampicillin to provide coverage of L. monocytogenes and S. agalactiae.
Cellulitis is an inflammation of the connective tissue underlying the skin, that can be caused by a bacterial infection.
Cellulitis
Bacterial Causes of Cellulitis • Staphylococcus aureus • Streptococcus pyogenes • Other streptococci 13 -37% 4 -17% 1 -18%
Treatment of Cellulitis
Treatment of Cellulitis • Mild Disease (oral formulations) – Antistaphylococcal penicillins (Dicloxacillin) – First Generation Cephalosporins (Cephalexin, Cefadroxil) – Clindamycin – Macrolides (Erythromycin, azithromycin, clarithromycin)
Treatment of Cellulitis • Severe Disease (intravenous formulations) – Antistaphylococcal penicillins (Nafcillin, oxacillin) – First-generation cephalosporins (cefazolin) – Clindamycin
Treatment of Cellulitis • If MRSA is suspected – Vancomycin – Linezolid – Daptomycin – Tetracyclines (Tigecycline, doxycycline) – Sulfa drugs (Trimethoprimsulfamethoxazole) – Clindamycin
• http: //www. virtualrespiratorycentre. com/ diseases. asp? did=879
Symptoms of Otitis Media • Otalgia (ear pain) • Hearing Loss • Irritability • Anorexia • Apathy • Fever • Swelling around the ear • Otorrhea (discharge from the affected ear)
Bacterial Causes of Acute Otitis Media • Streptococcus pneumoniae • Haemophilus influenzae • Moraxella catarrhalis 25 -50% 15 -30% 3 -20%
Treatment of Acute Otitis Media
Treatment of Acute Otitis Media • First Line Therapy – High Dose Amoxicillin • If Mild Allergy to Penicillin – Cefdinir, Cefpodoxime, Cefuroxime axetil • If Type 1 Hypersensitivity Allergic Reaction – Macrolide (Azithromycin, Clarithromycin, Erythromycin with sulfisoxazole)
Sulfmethoxazole Sulfisoxazole Used in combination with Erythromycin Used in combination with Trimethoprim (co-trimoxazole)
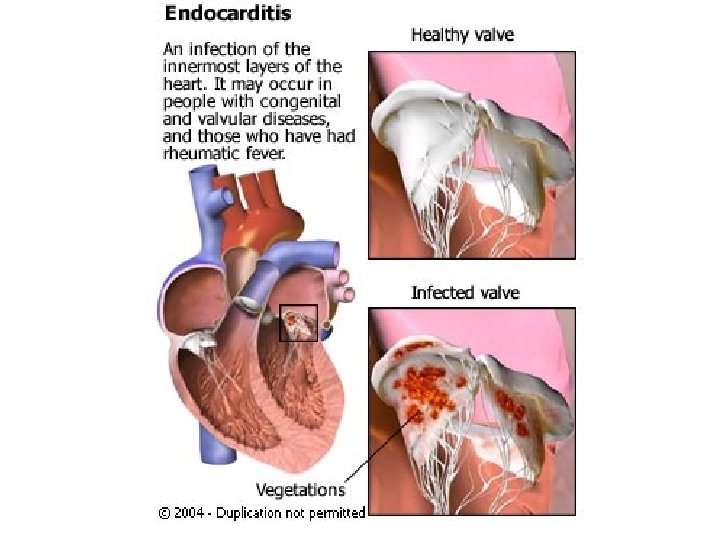
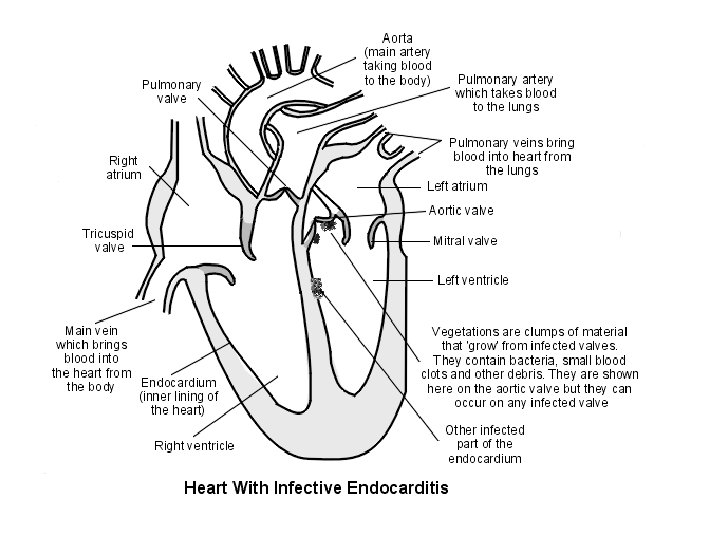
Infective Endocarditis
Causes of Endocarditis • There are many ways that bacteria can enter the bloodstream and cause endocarditis. Even a small cut can enable bacteria that normally live on the skin to enter the bloodstream.
• In some cases, this occurs during a dental or surgical procedure. In many cases, however, it is not clear how the bacteria first got into the bloodstream.
Symptoms of Endocarditis • Symptoms are non-specific, making endocarditis difficult to diagnose: • Fatigue • Malaise • Weakness • Weight loss • Fever • Chills • Dyspnea on exertion (shortness of breath)
Bacterial Causes of Endocarditis • • • Viridans group streptococci 18 -48% Staphylococcus aureus 22 -32% Enterococci 7 -11% Coagulase-negative staphylococci 7 -11% HACEK organisms 2 -7%
Viridans Group streptococci • Viridans streptococcus are alpha-hemolytic, normal flora of the oral, respiratory tract, and GI mucosa.
• They are the major cause of bacterial endocarditis in people with damaged heart valves. They may enter the blood stream after dental procedures.
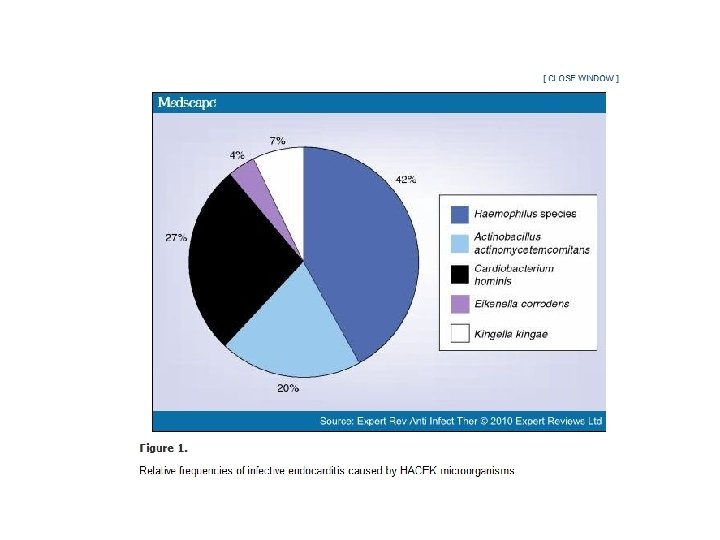
HACEK Organisms • A HACEK organism is one of a set of slow-growing Gram negative bacteria that form a normal part of the human flora. They are a frequent cause of endocarditis in children. • The name is formed from their initials: • Haemophilus aphrophilus, Haemophilus parainfluenzae and Haemophilus paraphrophilus • Actinobacillus actinomycetemcomitans • Cardiobacterium hominis • Eikenella corrodens • Kingella kingae
Empiric Therapy for Infective Endocarditis • Vancomycin + Gentamicin – Vancomycin is effective against S. aureus and viridans group streptococci – When used in combination with Gentamicin, activity is extended to the majority of enterococcal strains
• Even intensive therapy may not be sufficient, and surgical intervention is often required • Despite intensive antibiotic therapy, mortality remains high: 20 -25%.
Prosthetic Valve Endocarditis • Many cases of endocarditis are associated with prosthetic valves in the heart
• Sometimes these infections occur within two months after the valve is installed and are thus thought to be hospital acquired • Sometimes they occur 6 -20 month after surgery and are thus thought to be community acquired
Treatment of Prosthetic Valve Endocarditis • Vancomycin + Gentamicin + Rifampin – With or without cefepime or ceftriaxone
Intravascular-Related Catheter Infections • http: //www. skinisthesource. org/
• 200, 000 catheter-related infections occur each year in the U. S. • Should be suspected in anyone with an intravascular catheter and a fever of unclear etiology.
• Diagnosis may involve: – Removal and culture of the catheter – Growth of bacteria from blood cultures
What type of bacteria cause catheter-related infections? • Skin flora, including: – Staphylococcus epidermidis 32 -41% – Staphylococcus aureus 5 -14% – Enteric Gram-negative bacilli 5 -11% – Psuedomonas aeruginosa 4 -7%
Treatment of Intravascular Catheter-related Infections
Treatment of Catheter Related Infections • Hospital setting where MRSA is uncommon – Antistaphylocccal penicillin: Nafcillin, Oxacillin • Hospital setting where MRSA is common – Vancomycin • Immunocompromised or severely ill patient – Add cephalosporin to initial antibiotic regimen – Ceftazidime, cefepime
Intra-Abdominal Infections
Causes of Intra-abdominal infections • Usually caused by contamination of the usually sterile abdomen with microbial flora of the bowel • Can be quite severe, leading to sepsis and death
Bacterial Causes of Intraabdominal Infections • Gram-negative bacilli – Escherichia coli 32 -61% – Enterobacter spp. 8 -26% – Klebsiella spp. 6 -26% – Proteus spp. 4 -23%
Bacterial Causes of Intraabdominal Infections • Gram-positive cocci – Enterococci 18 -24% – Streptococci 6 -55% – Staphylococci 6 -16%
Bacterial Causes of Intraabdominal Infections • Anaerobic bacteria – Bacteroides spp. – Clostridium spp.
Treatment of Intra-abdominal Infections • Due to their polymicrobial nature, the antibiotic regimen must be very broad spectrum, including Gram-negative bacilli, Gram-positive cocci, and anaerobic bacteria
Treatment of Intra-Abdominal Infections • -Lactam/ -lactamase inhibitor combinations (piperacillin/tazobactam) • Carbapenems (imipenem, meropenem) • Aminoglycoside (gentamicin, tobramycin, amikacin) + metronidazole • Ciprofloxacin + metronidazole
Treatment of Intra-abdominal Infections