Integumentary StevensJohnson Syndrome SJS What is it a


 in some")

 and")













- Slides: 19
Integumentary Stevens-Johnson Syndrome SJS
What is it • a rare, serious disorder of the skin and mucous membranes • In adults its usually caused by a drug reaction • In children its usually caused by an infection • Lesions cover <10% • Mortality rate 5%
Pathophysiology • Theory: altered drug metabolism (eg, failure to clear reactive metabolites) in some patients triggers a T-cell– mediated cytotoxic reaction to drug antigens in keratinocytes – CD 8+ T cells have been identified as important mediators of blister formation
Pathophysiology • Theory: granulysin released from cytotoxic T cells and natural killer cells might play a role in keratinocyte death – Granulysin concentration in blister fluid correlates with severity of disease
Pathophysiology • Theory: interactions between Fas (a cell -surface receptor that induces apoptosis) and its ligand, particularly a soluble form of Fas ligand released from mononuclear cells, lead to cell death and blister formation
Toxic epidermal necrolysis TEN • • Severe form of SJS Cell-mediated cytotoxic reaction Lesions cover >30% of body Mortality rate is 40%
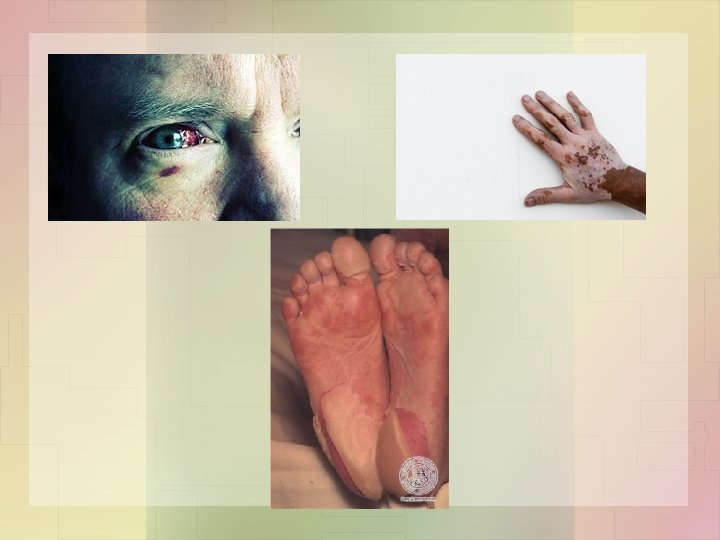
Clinical Manifestations • Within 1 to 3 wk after the start of the offending drug, patients develop a prodrome of malaise, fever, headache, cough, and keratoconjunctivitis • Macules, often in a target configuration, then appear suddenly, usually on the face, neck, and upper trunk
Clinical Manifestations • Macules simultaneously appear elsewhere on the body, coalesce into large flaccid bullae, and slough over a period of 1 to 3 days • Nails and eyebrows may be lost along with epithelium • The palms and soles may be involved
Clinical Manifestations • Skin, mucosal, and eye pain are common • In some cases, diffuse erythema is the first skin abnormality of toxic epidermal necrolysis
Clinical Manifestations • Skin is excruciatingly tender • Loss of skin leaves a weeping surface similar to a total-body, partial thickness burn
Severe TEN • large sheets of epithelium slide off the entire body at pressure points exposing weepy, painful, and erythematous skin • Painful oral crusts and erosions, keratoconjunctivitis, and genital problems accompany skin sloughing in up to 90% of cases
Severe TEN • Bronchial epithelium may also slough, causing cough, dyspnea, pneumonia, pulmonary edema, and hypoxemia • Glomerulonephritis and hepatitis may develop
Medical Management • Ophthalmology consultation and specialized eye care mandatory for patients with ocular involvement • Potentially causative drugs should be stopped immediately • Patients are isolated to minimize exposure to infection
Medical Management • Fluids, electrolytes, blood products, and nutritional supplements as needed • Skin care includes prompt treatment of secondary bacterial infections and daily wound care as for severe burns • Prophylactic systemic antibiotics are controversial and often avoided
Nursing Interventions • Skin assessment – Monitor for infection – Monitor for development of new blisters – Monitor the amount and characteristics of blister drainage • Oral assessment – Blistering and erosive lesions – Ability to swallow and drink fluids – Ability to speak normally
Nursing Interventions • Assess for itching, burning, and dryness of the eyes – Monitor for conjunctival hemorrhage • Vital signs • Respiratory assessment
Watch for • High fever, tachycardia, and extreme weakness and fatigue may indicate the process of epidermal necrosis, and GI and respiratory mucosal sloughing • Daily assessment of puncture sites and IV sites for oozing • Careful assessment of GU system • Daily weights
Nursing Diagnoses • Impaired tissue integrity r/t epidermal shedding • Fluid volume deficit • Electrolyte imbalance • Impaired thermoregulation • Acute pain • Anxiety • Impaired mobility • Nutrition less than body requirements