Hypothalamic Pituitary Hormones Dept of Pharmacology CIPS The




 –")




. 2 - Prolactin")
 • 44 amino acid peptide • Full biological activity in")
 • Structure- 14 - or 28 -amino acid structure • Function –")
 • Somatostatin analogue. • 8 amino acid derivative of somatostatin that preferentially")

: • Structure: It is a single polypeptide chain composed of 191")

 : GH SUPPLEMENTATION Somatropins GH preparations")









")



 from the anterior pituitary")
- Slides: 32
Hypothalamic Pituitary Hormones Dept. of Pharmacology, CIPS
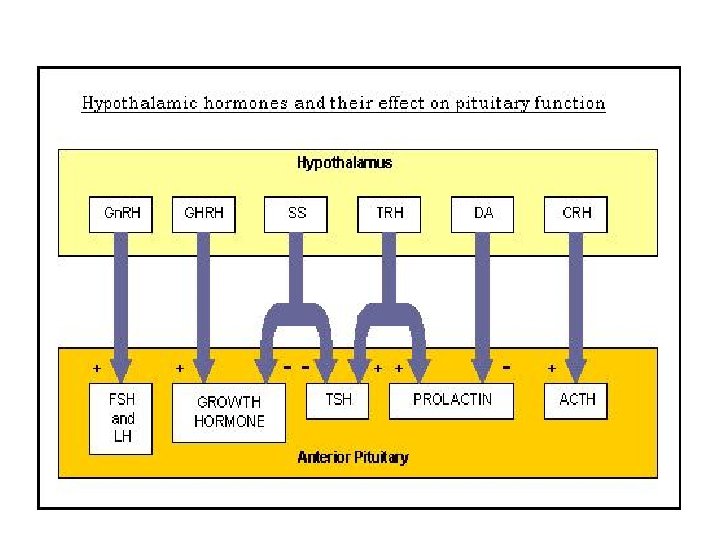
The hypothalamic - pituitary axis: • The pituitary is connected to the hypothalamus by a stalk (the infundibulum) which carries axons to the neurohypophysis (posterior pituitary) as well as blood vessels to the adenohypophysis (anterior pituitary). • Most feedback loops run through this axis • HPA mediates Reproduction. Growth, Metabolism, Stress response,
The Hypophyseal Portal System
Characteristics of Hypothalamic releasing and inhibiting hormones • Hypothalamic releasing and inhibiting hormones are carried directly ONLY to the anterior pituitary gland via hypothalamic hypophyseal portal veins. • Secretion is pulsatile • They have short half lives so their actions on the pituitary are of short duration. • Their actions are limited by negative feedback mechanisms. • They stimulate release of anterior pituitary hormones. • They stimulate synthesis of anterior pituitary hormones. • They stimulate hyperplasia and hypertrophy of target cells.
Hypothalamic Neurohormones Seven neurohormones are made in the hypothalamus – Thyrotropin-releasing hormone (TRH) – Corticotropin-releasing hormone (CRH) – Gonadotropin-releasing hormone (Gn. RH) – Growth hormone-releasing hormone (GHRH) – Growth hormone-release inhibiting hormone (GHIH) or somatostatin – Prolactin-releasing factor (PRF) – Prolactin-inhibiting hormone (PIH)
Negative Feedback Inhibition Hormone Homeostasis. Maintenance of hormone levels within a particular physiological range
Anterior Pituitary
Control of Anterior Pituitary • It has no neural connection with the hypothalamus • There is a capillary plexus in the hypothalamus • It gives rise to the Hypothalamo-hypophyseal portal system • Neurohormones from hypothalamus pass through this portal system to stimulate or inhibit the anterior pituitary Control of Posterior Pituitary • Neurons arising in : Ø Paraventricular nucleus Ø Supraoptic nucleus § Sends neurons down pituitary stalk (infundibulum) § They synapase with capillaries in the posterior pituitary § Secrete the neurohormones Oxytocin and vasopressin A § Directly into the blood stream
Posterior Pituitary
Anterior pituitary hormones: • Somatotropic Hormones: 1 - Growth Hormone (GH). 2 - Prolactin (Prl). 3 - Placental Lactogen (PL). • Glycoprotein Hormones: 1 - Luteinizing Hormone (LH). 2 - Follicle-Stimulating Hormone (FSH). 3 - Chrionic Gonadotropin (CG). 4 - Thyroid-Stimulating Hormone (TSH). • Pro-Opio melano cortin (POMC) derived Hormones: 1 - Corticotropin: ACTH. 2 - Melanocyte-Stimulating Hormones: a-MSH, b-MSH. 3 - Lipotropins: b-LPH, -LPH
Growth Hormone-Releasing Hormone (GHRH) • 44 amino acid peptide • Full biological activity in 1 -29 – Structural homologies to GI peptide hormones • Function – Stimulates synthesis and release of growth hormone (GH) from the anterior pituitary • Research purposes only – IV, Sub. Q or intra-nasally. – IV half life is 4 minutes Growth Hormone-Releasing peptides (GHRPS) • Group of synthetic peptide analogues that can stimulate GH secretion • Sermorelin {Geref} --Used as diagnostic agent. – Must have properly functioning pituitary.
Somatostatin (GHIH) • Structure- 14 - or 28 -amino acid structure • Function – Inhibits growth hormone release in normal individuals, thus opposes GHRH – Inhibits the release of glucagon, insulin TSH, LH and gastrin (GI hormones) – Lowers the rate of gastic empting and reduces smooth muscle contractions and decreases blood flow of the intestine • Half life 1 -3 minutes • Kidney is key in metabolism and elimination SOMATOSTATIN (SS) ANALOGUES Drug Type Dosing Octreotide Short-acting SC 3 times/day; dose range of 50 -500 mg Octreotide LAR Long-acting IM every 28 days; dose range of 10 -40 mg Lanreotide depot Long-acting IM every 7 -14 days, 30 mg. Lanreotide autogel Long-acting Deep SC every 28 days, supplied in prefilled syringes containing 60/90/120 mg
Octreotide (SANDOSTATIN) • Somatostatin analogue. • 8 amino acid derivative of somatostatin that preferentially binds to SS receptors on GH-secreting tumors. • Inhibits release of GH from pituitary • Pharmacokinetics • Half life of 80 minutes • Administered SC or IM. • 45 x more potent than endogenous peptide • Therapeutic use • Treatment of a variety of hormone-secreting tumors • Acromegaly • Adverse reactions • Biliary tract abnormalities • Gallstones, sludge without stones, biliary duct dilation • Bradycardia, nausea, vomiting, abdominal cramps, flatulence
• Induces lipolysis in adipose tissue and growth in skeletal muscle – Binding to its receptor (direct) • Adipose tissue stimulated to break down triglyceride and stops the uptake of circulating lipids – Insulin-like growth factor-1 (indirect) • Stimulates the liver to release IGF-1 target tissues>produces growth at open epiphyses • Lanreotide (SOMATULINE-LA) slow release, long-acting octapeptide causes • prolonged GH suppression. Most effective for patients with nonpituitary tumours
Growth Hormone (GH): • Structure: It is a single polypeptide chain composed of 191 amino acid residues. It has two disulfide bonds. • Secretion: Somatotropes of the Anterior Pituitary. • Level: High in children Maximal during adolescence Lowest during adulthood. • Measurments: During 24 hours After stimulation • Regulation: Stimulation: By Growth Hormone Releasing Hormone (GHRH). Inhibition: By Somatostatin. • Direct Effects: 1 - Stimulation of Lipolyses (Hydrolyses of Triglycerides). 2 - Stimulation of Hepatic glucose output. 3 - Production of Insulin-like growth factors (IGF’s, Somatomedins) • Indirect Effects: Mediated by IGF-1: 1 - Increase cell numbers. 2 - Positive Nitrogen balance. 3 - Increase Protein synthesis.
Disease Conditions Related to GH: • Deficiency: * Dwarfism. • Excessive Secretion: * Giantism: Due to tumor in somatotrpes in young children or adolescents. * Acromegaly: Rare disease (3/Million). Causes: 1 - Benign tumor of Pituitary gland (90%). 2 - Tumors of pancreas, lung or adrenal Symptoms: Enlargements of extremities. • Uses of Growth Hormone: * Replacement therapy for children with GH deficiency. * Administered by intramuscular or subcutaneous. • Sources: * Recombinant DNA technology.
Treatment of GH insufficiency (all SC or IM) : GH SUPPLEMENTATION Somatropins GH preparations whose sequence matches native h. GH. Somatrem: GH derivative with an additional methionine at the amino terminus. For Children • To mimic the normal pattern of secretion, they typically are administered to GH-deficient children in a dose of 40 mg/kg per day subcutaneously in the evening; • Higher daily doses (e. g. , 50 mg/kg) are employed for patients with Turner's syndrome, who have partial GH resistance. • In children with overt GH deficiency, measurements of serum IGF-1 levels are used to monitor initial response and compliance; long-term response is monitored by close evaluation of height For adults, the FDA recommends a starting dose of 3 to 4 mg/kg, given once daily by subcutaneous injection, with a maximum dose of 25 mg/kg in patients £ 35 years old and 12. 5 mg/kg in older patients.
Side Effects of GH Therapy: In children: • GH therapy is associated with remarkably few side effects. • Rarely, intracranial hypertension, visual changes, headache, nausea, and/or vomiting. • Leukemia has been reported in some children receiving GH therapy; and conditions associated with GH deficiency (e. g. , Down's syndrome, cranial irradiation for CNS tumors) probably explain the apparent increased incidence of leukemia. • An increased incidence of type 2 diabetes mellitus has been reported. In adults • Side effects associated with the initiation of GH therapy include Peripheral edema, carpal tunnel syndrome, arthralgia, and myalgia. • These symptoms, which occur most frequently in patients who are older or more obese, generally respond to a decrease in dose.
IGF-1 THERAPY For Pts with GH Receptor mutation Mecasermin: complex of recombinant human IGF-1 (rh. IGF-1) and recombinant human insulin-like growth factor-binding protein-3 (rh. IGFBP-3). Clinical response is monitored Serum IGF-1 levels. Treatment of Acromegaly: Trans-sphenoidal surgery to remove tumor. Radiation therapy usually follow the surgery. Drug Therapy: 1 - Dopaminergic Agonists: Bromocriptine 2 - Synthetic Somatostatin analogs: Octeroide (Sandostatin).
Growth Hormone Receptor Antagonist: • Binds to GH receptors, blocks GH-stimulated, hepatic production of IGF-1 • Pegvisomant {Somavert} • Injection, SC. • Treatment of – Acromegaly • Increased growth hormone in adults • Adverse reactions – Pain/redness/itching at the injection site, diarrhea, or nausea may occur. – Liver toxicity, yellowing of the skin, abdominal pain, dark urine, vomiting – Allergic reactions • CI – Liver disease
Prolactin: • 198 amino acid peptide with three disulfide bonds • Lactation • Recombinant agents not available • Hypothalamic dopamine inhibits the secretion and release of prolactin. • Major function of prolactin is milk production – oxytocin stimulates ejection • Release is tonically inhibited by PIH (dopamine) • Suckling response inhibits PIH release Other Physiological Roles of Prolactin: – important for reproduction - female – produced in uterine – endometrium during menstrual cycle – male – absence decreases fertility – involved in immune system – involved in T lymphocyte differentiation
Hyperprolactinemia • Galactorrhea • Amenorrhea • Male impotence • Associated with autoimmune diseases: multiple sclerosis, lupus Dopamine Agonists: • Decrease prolactin secretion through a dopamine-mimic action • Bromocriptine –D 2 receptor agonist, D 1 anta. • Pergolide • Cabergoline • Quinagolide –Non ergot dopamine agonist. Oral administration Treatment of Prolactin secreting adenomas Acromegaly Parkinson’s disease Adverse reactions Headache, light headedness, fatigue, Psychotic reactions
Glycoprotein hormones: Ø LH, FSH, TSH and h. CG Ø a and b subunits Ø Each subunit encoded by different gene Ø a subunit is identical for all hormones Ø b subunit are unique and provide biological specificity Gonadotropin-Releasing Hormone – Pulsatile Gn. RH secretion stimulates the gonadotroph cells in the anterior pituitary to produce and release LH & FSH • Sustained non-pulsatile administration inhibits the release of FSH and LH by the pituitary in both males and females
Gonadorelin {Factrel}: • Synthetic Gn. RH - Small peptide • Diagnostic purpose only • Portable pump system - Male and female infertility • Administered SC and IV Gn. RH Analogs: • Synthesized by selective substitution of amino acids • Leuprolide {Eligrad} – Highly effective at decreasing estrogen levels – Given IM/SC. • Nafarelin {Synrel} – Nasal spray • Goserelin {Zoladex} – Implantable cylinders Histrelin, Triptorelin.
• Treatment of – Endometriosis and Uterine fibroids – Breast cancer – Prostate cancer – Central precocious puberty – Male and female infertility • Adverse reactions – Hot flashes, acne, depression, vaginal bleeding – Tachycardia, lightheadedness, ED • Gn. RH Antagonist • Binds to pituitary Gn. RH receptors without activation – Blocks secretion and release of LH and at high doses FSH – Immediate suppression of LH • Ganirelix {Antagon} • Cetrorelix {Cetrotide}
• Treatment of – In vitro fertilization – Endometriosis and uterine fibroids • Advantage – Decrease risk of LH surge • Injectables SC. • Adverse reactions – Nausea – HRs. – Vaginal bleeding Follicle Stimulating Hormone: • Glycoprotein hormone consisting of two chains • Produced by gonadotroph cells in the anterior pituitary • Stimulates gametogenesis and follicular development in women and spermatogenesis in males • Stimulates androgen conversion into estrogen
Menotropin {Humegon}: • Commercially available since 1960 s • human Menopausal Gonadotropins (h. MG) – Purified from urine of post-menopausal females • Combination of FSH and LH • MENOPAUSE happens when no follicles remain in the ovaries – ESTROGEN and PROGESTERONE are no longer made, thus leading to high levels of circulating FSH and LH Urofollitropin {Bravelle} • Purified FSH • Derived from post-menopausal females Follitropin Beta {Follistim} • 1996, recombinant technology • Batch to batch consistency, and highly pure • Cost 3 x as much as h. MG • Injectables, SC. • Treatment: Anovulatory females; Pituitary and hypothalamic hypogonadism with infertility
• Adverse reactions – Abdominal pain, vaginal bleeding, ovarian cysts – Injection site pain, rash • Risk of multiple births Luteinizing Hormone • Glycoprotein consisting of two chains • Regulation of gonadal steroid production • No LH clinically available • human Chorionic Gonadotropin (h. CG) – IM injection – Half life of 8 hours Human Chorionic Gonadotropin (h. CG): • Diagnostic use • Treatment of infertility – Induce ovulation • Adverse reactions – Headache – Depression
ACTH is made up of 39 amino acids Ø Regulates adrenal cortex and synthesis of adrenocorticosteroids Ø a-MSH resides in first 13 AA of ACTH Ø a-MSH stimulates melanocytes and can darken skin Ø Overproduction of ACTH may accompany increased pigmentation due to a-MSH. Regulation of ACTH: • Stimulation of release – CRH and ADH – Stress – Hypoglycemia • CRH and ADH both synthesized in hypothalamus – ADH is released by posertior pituitary and reaches anterior pituitary via inferior hypophyseal artery.
Corticotropin-Releasing Hormone: • Secreted in response to stress • Stimulates corticotropin cells to produce adrenocorticotropic hormone (ACTH) • Diagnostic use only Thyroid Stimulating Hormone: TSH • Thyrotrophs: Thyroid Stimulating Hormone (TSH) • Hypothalamic Control Thyrotropin Releasing Hormone (TRH) • Target Tissue Follicular cells of the Thyroid gland • Hormone effects: controls the production of T 3 and T 4
Thyrotropin-Releasing Hormone: • Stimulates secretion of thyroid stimulating hormone (TSH) from the anterior pituitary • Protirelin {Relefact TRH} • Diagnostic purposes only Hormone + Receptor